Tremor is one of the most common movement disorders. The tremor can be so pronounced that it significantly impairs the quality of life for those affected. Tremor patients often find it impossible to perform everyday tasks, such as drinking from a glass, shaving, or writing legibly. There are various treatment options for these significant limitations. For instance, many forms of tremor respond excellently to deep brain stimulation. In the following, we delve into the specific tremor disorders and the treatment recommendations from our specialists at Inselspital.
What is tremor?
Tremor is an involuntary, rhythmic oscillation of one or more body parts. The hands, arms, legs or vocal cords can be affected. It is important to note that tremor is only a symptom. The causes of tremor can be very different. That is why a classification is also so difficult *.
What are the different types of tremor?
Tremors can affect different parts of the body. Accordingly, we then speak of hand tremors, arm tremors, leg tremors or head tremors. Even the vocal cords may be affected. Vocal tremors cause a shaky voice that is sometimes difficult to understand.
The tremors may also only occur in certain situations and be absent in others. A distinction is made here between, among other things, a resting tremor, which occurs during physical relaxation, and an action tremor, which becomes apparent during purposeful movements.
Based on the combination of tremor characteristics and other neurological findings, the physician may combine the tremor into a tremor syndrome. This distinction is very important with regard to further treatment options, since the individual forms of tremor respond very differently to different forms of treatment.
Some forms of tremor respond very well to surgical therapy. In the following, we will discuss these subtypes in more detail:
Essential tremor
This common tremor disorder (affecting approximately 4–5% of individuals over the age of 65) can occur in adolescence or manifest later in life, but it typically starts around the age of 40. In slightly more than half of the cases, a genetic cause is suspected due to a family history of tremor or a parent also being affected. However, no responsible gene has been identified yet.
Essential tremor usually progresses over time, meaning it becomes stronger as time goes on. Clinically, it mainly presents as postural and action tremor. Typically, the arms and hands are steady when relaxed, without any shaking. However, when purposeful movements involving the arms and hands are attempted or when the affected body parts are held, a medium-frequency tremor (5–8 Hz) occurs. Usually, both sides of the body are affected. Just over half of the individuals report a reduction in tremor intensity after consuming alcohol.
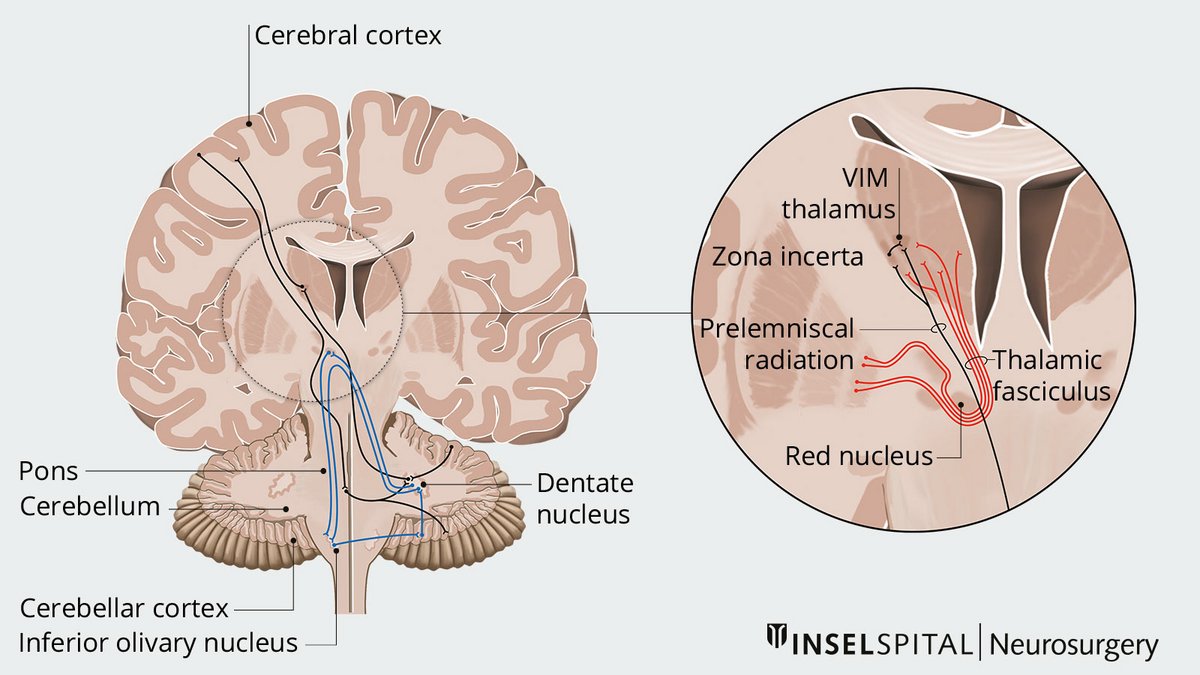
Our illustration provides a schematic overview of the structures involved in tremor formation. The cerebellum, thalamus, brainstem nuclei, and the fiber pathways connecting these regions, such as the dentatorubrothalamic tract, play a central role in this process.
Parkinson's disease tremor
Tremor in Parkinson's patients is typically a resting tremor. This is otherwise found almost exclusively in Holmes tremor and dystonic tremor. The presence of a classic, unilateral (affecting one side of the body), low-frequency resting tremor is one of the most reliable criteria for diagnosing Parkinson's disease because over 90% of Parkinson's patients suffer from this form of tremor. Resting and postural tremors are less common in Parkinson's.
Holmes tremor
This form of tremor is clinically defined as a slow-frequency resting and intention tremor in patients with brain lesions. The period from the causative brain lesion to the onset of the first symptoms can range from several weeks to years. Intention tremor refers to a tremor that occurs during a purposeful movement. It is easiest to observe in the hands when reaching for an object, as the tremor becomes stronger as the hand approaches the object. The most common causes of Holmes tremor include multiple sclerosis, brain trauma, and ischemic brain lesions.
Dystonic tremor
This tremor, characterized by variable frequency (around 3–7 Hz), affects one limb or body part displaying at least minimal signs of dystonia. Resting, postural, and action tremors are rare. Diagnostic challenges arise in cases where the tremor precedes dystonia.
What are the treatment options?
The treatment of tremors depends largely on the underlying disease. Diagnosis and therapy are carried out by neurologists with experience in the field of movement disorders. The corresponding experts at Inselspital can be found at the Center for Parkinson's Disease and Movement Disorders (ZfPB).
Drug therapy
Drug therapy is the treatment of choice *:
- Essential tremor initially should be treated with primidone or propranolol, a beta-blocker, or a combination of both. Efficacy and side effects limit their use. Topiramate and gabapentin have good success in some patients and should be used as second-line therapy.
- Parkinson's disease tremor usually improves with proper dopaminergic therapy to treat akinesia and rigor. If the tremor remains unchanged, anticholinergics (e.g. biperides), propranolol, or clozapine can be tried.
- There is no established drug therapy for Holmes tremor, and medication treatment for Holmes tremor has rarely been successful. In isolated cases, success of L-dopa, levetirazetam, clonazepam, and clozapine is observed.
- There is also no established drug therapy for dystonic tremor. Medication treatment is based on expert opinion. Trihexyphenidyl, propranolol, lioresal, and clonazepam are suggested.
Deep brain stimulation or lesioning – modern treatment options for tremor
When medications provide only limited relief or cannot be used due to side effects or intolerance, functional neurosurgical treatments may offer a promising alternative.
Two main surgical options are available:
- deep brain stimulation (DBS)
- lesioning procedures, such as thalamotomy with high-intensity focused ultrasound (HIFU)
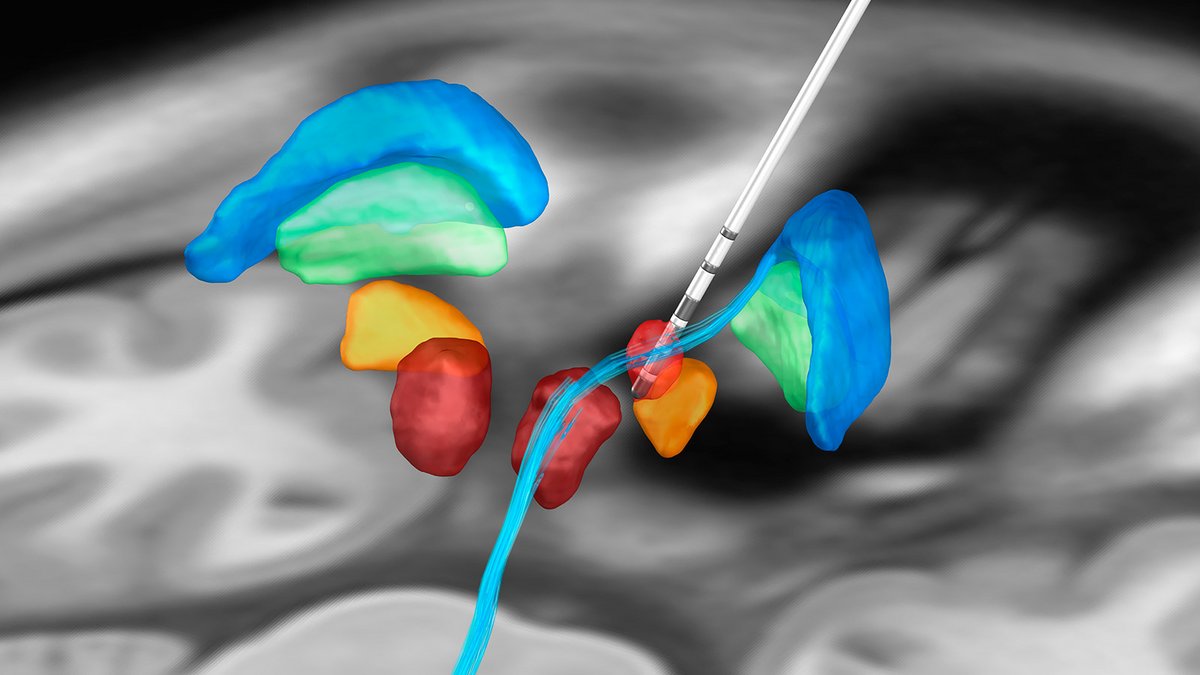
DBS is currently one of the most effective and adaptable treatments for essential tremor and Parkinsonian tremor.Electrodes are implanted into specific areas of the brain, where controlled electrical impulses help suppress tremor symptoms. One of the key advantages of DBS is its flexibility: the stimulation can be precisely adjusted to individual needs and, unlike lesioning, is reversible. Side effects such as speech disturbances or balance issues are less common and often reversible with DBS. *, *, *.
The ventral intermediate nucleus (VIM) of the thalamus and the posterior subthalamic area (PSA) are well-established targets for treating essential tremor. A randomized study has demonstrated the superiority of DBS over thalamotomy (surgical lesioning of the thalamus) in terms of side effects *.
While both approaches are effective in tremor suppression, they differ significantly regarding potential side effects. DBS is associated with fewer risks of speech impairment, imbalance, sensory disturbances or cognitive side effects – and most of them are reversible.
At Inselspital, DBS is typically the preferred treatment for suitable candidates. However, in select cases, thalamotomy via MR-guided focused ultrasound (MRgFUS) can be a valuable alternative. This non-invasive option is particularly appealing for patients who may not be eligible for surgery or prefer not to undergo an invasive procedure. However, it’s important to note that lesioning effects are permanent, and any potential side effects cannot be reversed. *
Which method is right for you? Our experienced team will help you decide based on your medical needs and individual situation.
How is deep brain stimulation used for tremor?
In Parkinson's patients, three target structures in the brain can be successfully stimulated in principle and must be discussed individually for each patient in our expert board:
- Stimulation in the area of the nucleus subthalamicus is most frequently selected because akinesia and rigor can also be successfully treated by stimulation and the amount of medication can usually be considerably reduced. A potential disadvantage is the worsening of pre-existing core instability, the so-called postural instability.
- According to the latest studies, GPi stimulation is currently considered to be equivalent *.
- In rare cases of pure tremor dominance of the Parkinson's patient in advanced age, stimulation in the motor thalamus (VIM) or posterior subthalamic area (PSA) is used. This is because patients have a more rapid onset of action with fewer complications after VIM stimulation and usually do not experience the late stages with very slow progression in advanced age.
The data is less obvious for other forms of tremors such as Holmes tremor and dystonic tremor. Case descriptions and series suggest good tremor reduction averaging over 70% in Holmes tremors *, with lesser results in dystonic tremor *.
In any case, any forms of these tremors should be discussed in an interdisciplinary way. In any case, the possibilities of deep brain stimulation in patients with severe forms of these tremors should be discussed on an interdisciplinary basis.
Based on the analysis of our published results from 2018, we achieve an average tremor reduction of 55–72% at Inselspital depending on the underlying disease and tremor subtype *, *.
What are the side effects of deep brain stimulation?
Generally, the same side effects apply as with all stereotactic functional DBS procedures. Specific risks associated with PSA stimulation for the treatment of tremor may include muscular twitching or cramping, speech disorders, or sensory insensitivity. Speech disorders are the most common side effect. However, these stimulation-induced side effects are usually reversible.
Why you should seek treatment at Inselspital
Like other disorders, the indication for DBS is generally made on an interdisciplinary basis by neurologists and neurosurgeons. Extensive examinations such as neurological examinations, neuropsychological tests, a psychiatric evaluation, and a surgical evaluation are performed in advance. The aim of this is to ensure that only patients with very good prospects of improving their symptoms are selected for the procedure. At Inselspital, patient cases are discussed individually by our interdisciplinary Movement Disorders Board in order to offer the best therapeutic options to each individual patient.
DBS surgery is a technically very complex procedure that is only offered in a few specialized centers. With just over 40 procedures of this type per year, Inselspital is the leader in Switzerland. Our specialists possess the necessary expertise and experience to successfully perform this very complex modern surgical technique. It is important to us that, despite all the modern technology and innovative procedures, our patients and their individual needs always remain the focus.
-
Deuschl, G., Bain, P. & Brin, M. Consensus statement of the Movement Disorder Society on Tremor. Ad Hoc Scientific Committee. Movement disorders : official journal of the Movement Disorder Society 1998;13 Suppl 3, 2-23.
-
Deuschl, G. et al. A randomized trial of deep-brain stimulation for Parkinson's disease. The New England journal of medicine. 2006;355, 896-908.
-
Odekerken, V. J. et al. Subthalamic nucleus versus globus pallidus bilateral deep brain stimulation for advanced Parkinson's disease (NSTAPS study): a randomised controlled trial. Lancet neurology 2013;12, 37-44.
-
Limousin, P., Speelman, J. D., Gielen, F. & Janssens, M. Multicentre European study of thalamic stimulation in parkinsonian and essential tremor. Journal of neurology, neurosurgery, and psychiatry 1999;66, 289-296.
-
Schuurman, P. R. et al. A comparison of continuous thalamic stimulation and thalamotomy for suppression of severe tremor. The New England journal of medicine 2000;342, 461-468.
-
Elias, W. J. et al. A Randomized Trial of Focused Ultrasound Thalamotomy for Essential Tremor. The New England journal of medicine 2016;375, 730-739.
-
Fiechter, M. et al. Deep Brain Stimulation for Tremor: Is There a Common Structure? Stereotactic and functional neurosurgery 2017;95, 243-250.
-
Nowacki, A. et al. Targeting the posterior subthalamic area for essential tremor: proposal for MRI-based anatomical landmarks. Journal of neurosurgery 2018;1-8.
-
Odekerken, V. J. et al. Subthalamic nucleus versus globus pallidus bilateral deep brain stimulation for advanced Parkinson's disease (NSTAPS study): a randomised controlled trial. Lancet neurology 2013;12, 37-44.
-
Mendonca, M. D., Meira, B., Fernandes, M., Barbosa, R. & Bugalho, P. Deep brain stimulation for lesion-related tremors: A systematic review and meta-analysis. Parkinsonism & related disorders 2018;47, 8-14.
-
Cury, R. G. et al. Thalamic deep brain stimulation for tremor in Parkinson disease, essential tremor, and dystonia. Neurology 2017;89, 1416-1423