Trigeminal neuralgia causes brief, intense, lightning-like shooting pains in the face, which usually occur on one side and recur. These pain attacks can significantly impair quality of life. The condition is often caused by contact between the trigeminal nerve and an adjacent blood vessel. The diagnosis is made based on typical symptoms and magnetic resonance imaging (MRI). If medication does not adequately relieve the pain, various neurosurgical treatment options are available.
How common is trigeminal neuralgia?
Trigeminal neuralgia is a rare condition. Each year, about 10 out of every 100,000 people are newly diagnosed with it. While it can affect anyone, women are affected slightly more often than men (ratio of about 1.8 to 1). The condition most commonly occurs between the ages of 70 and 80.
What are the symptoms of trigeminal neuralgia?
Trigeminal neuralgia is typically characterized by sudden, shooting, very severe pain in the middle to lower half of the face. The attacks always occur on one side, usually last only a few seconds, and can occur multiple times a day—up to a hundred times. Between pain attacks, those affected are generally symptom-free.
The pain is often triggered by everyday stimuli such as speaking, chewing, being touched, brushing teeth, or a draft. Since the pain often radiates into the jaw, it is frequently misinterpreted at first as a dental problem. As a result, many patients have already undergone dental examinations or treatments before the correct diagnosis is made.
The high intensity of the pain can significantly impair quality of life. Over time, dull, persistent pain may also develop, which can result from damage to the nerve fibers.
What are the causes of trigeminal neuralgia?
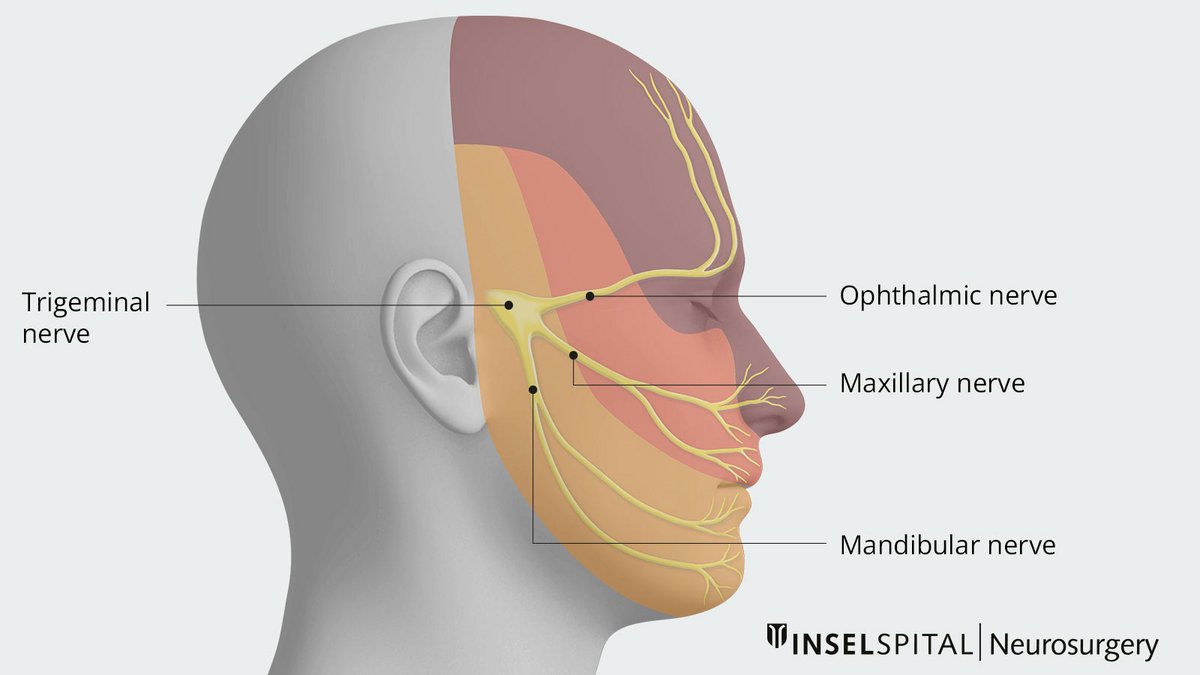
The trigeminal nerve (nervus trigeminus, 5th cranial nerve) is a nerve divided into three main branches and is responsible for sensation in the face and, to some extent, for the masticatory muscles. In trigeminal neuralgia, the pain is caused by a disruption of the sensory nerve fibers, usually in the middle and lower halves of the face.
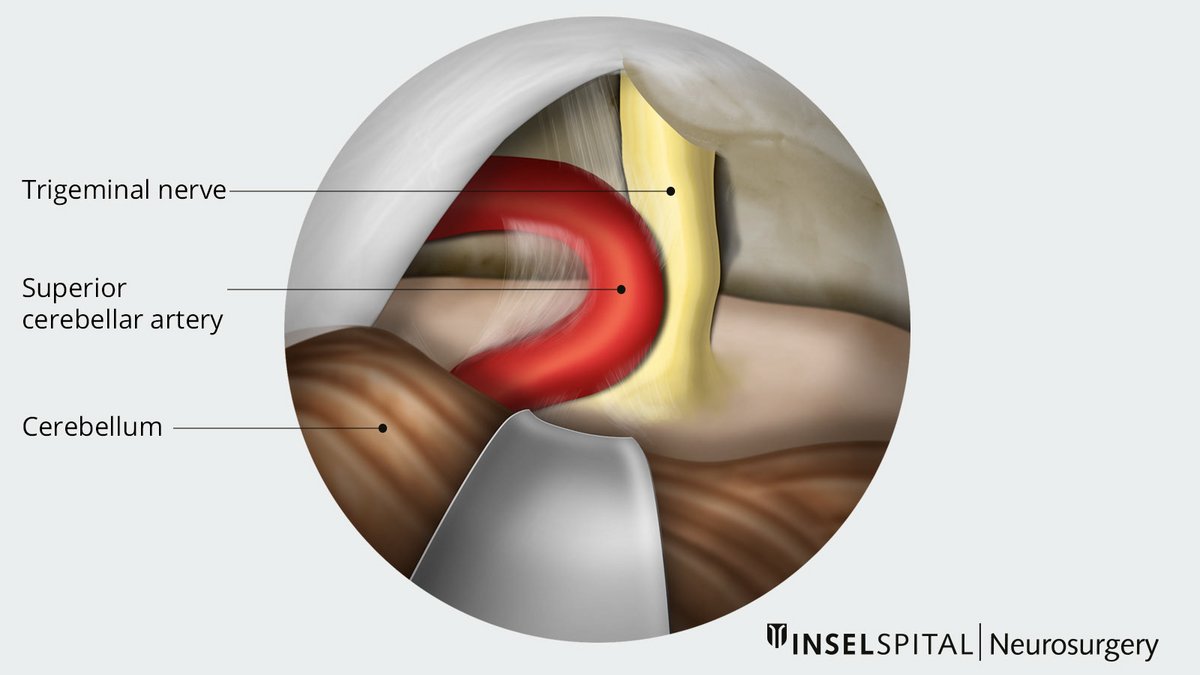
The most common cause is what is known as a neurovascular conflict («Jannetta mechanism»). In this condition, the trigeminal nerve is irritated by an adjacent, pulsating blood vessel. Prolonged contact can damage the protective nerve sheath, leading to the erroneous transmission of pain signals.
Such vascular contact is not always detectable on imaging. Conversely, it occurs in many people without causing any symptoms.
Less commonly, a condition known as symptomatic trigeminal neuralgia is present. In these cases, other conditions are the cause, such as a tumor near the nerve, inflammation, or multiple sclerosis.
How is trigeminal neuralgia diagnosed?
The diagnosis can often be made clinically based on the typical symptoms. To confirm the diagnosis and rule out other causes, a magnetic resonance imaging (MRI) scan of the skull is usually performed.
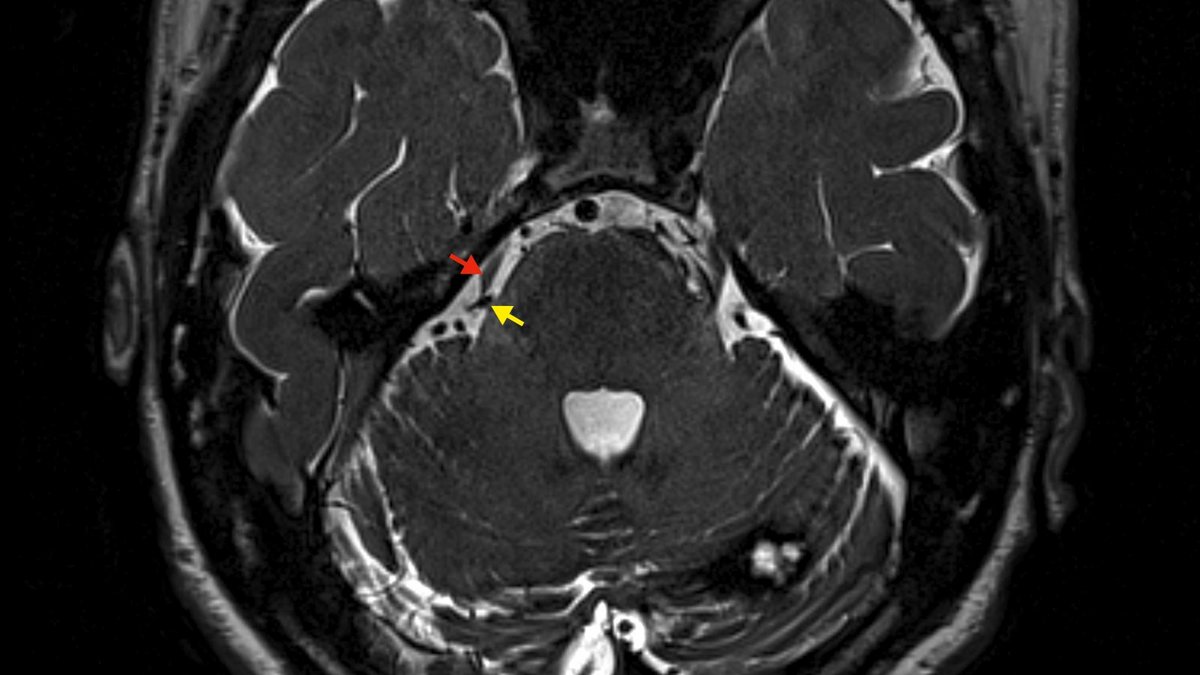
Specialized MRI images can provide a detailed view of the course of the trigeminal nerve. In many cases, these images can also reveal a neurovascular conflict, in which a blood vessel is irritating the nerve.
Conservative treatment
For many patients, medication can provide significant pain relief or even complete freedom from pain. Commonly used medications include carbamazepine, pregabalin, gabapentin, and baclofen. Treatment typically begins with a low dose, which is gradually adjusted. In some cases, a combination of different medications may be appropriate.
If pain cannot be adequately controlled despite medication or if significant side effects occur, invasive treatment should be considered.
Microvascular decompression (Jannetta surgery)
If medication does not adequately relieve the pain or is not tolerated, Jannetta microvascular decompression is considered the treatment of choice for classic trigeminal neuralgia.
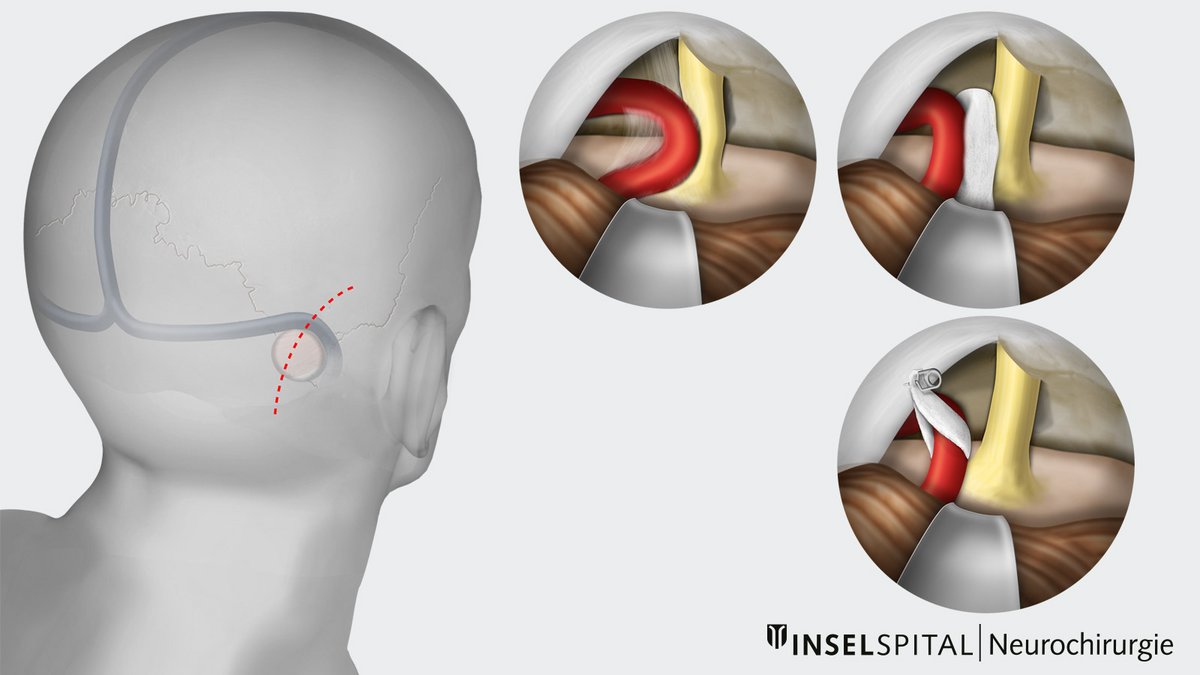
In this microsurgical procedure, the trigeminal nerve is exposed through a small incision behind the ear (retrosigmoid approach). The goal of the surgery is to relieve pressure on the nerve caused by an adjacent blood vessel that is irritating it. To do this, the vessel is carefully separated from the nerve and permanently kept at a distance using a small Teflon pad.
Even if no clear neurovascular conflict is visible on an MRI, it can often be identified and treated during surgery.
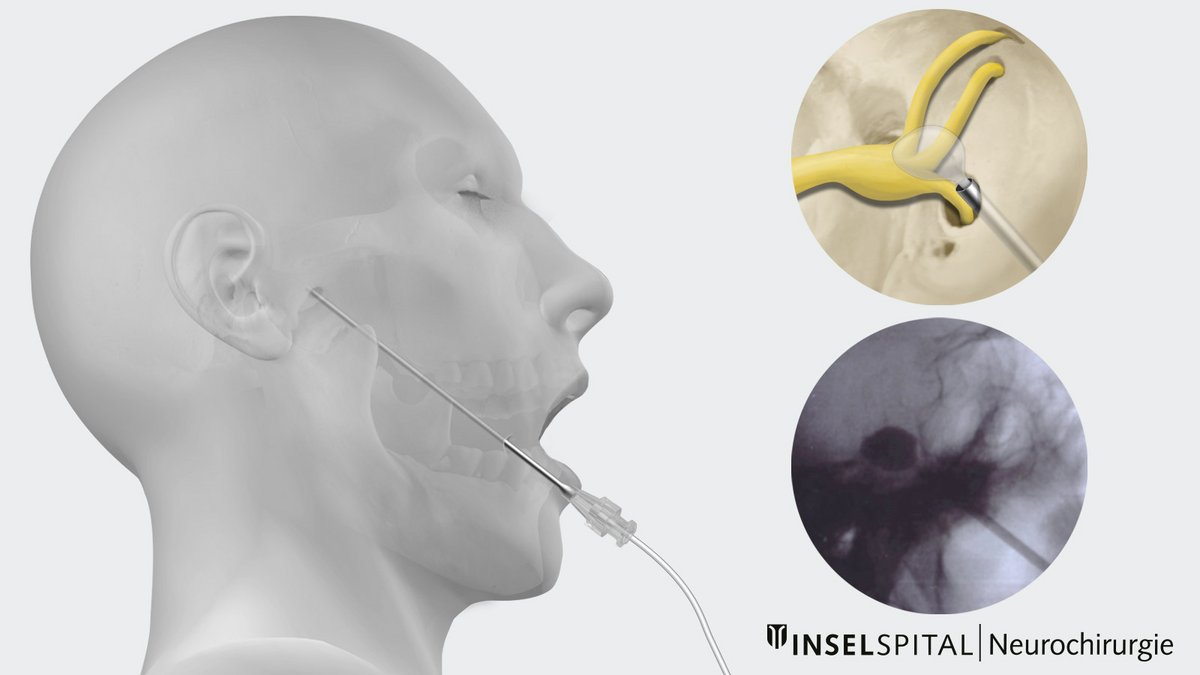
Balloon compression
Balloon compression is a minimally invasive procedure for treating trigeminal neuralgia. It is particularly suitable when medication is not sufficiently effective or when there is an increased risk associated with surgery or anesthesia due to age or other medical conditions. This procedure may also be a suitable treatment option for symptomatic trigeminal neuralgia—for example, in connection with multiple sclerosis—or in cases where symptoms recur after Jannetta surgery.
The procedure is performed under general anesthesia. A thin catheter is advanced through the cheek to the trigeminal ganglion. There, a small balloon is inflated for a short time. The resulting pressure selectively interrupts the transmission of pain signals and can thus effectively relieve symptoms.
Stereotactic radiosurgery
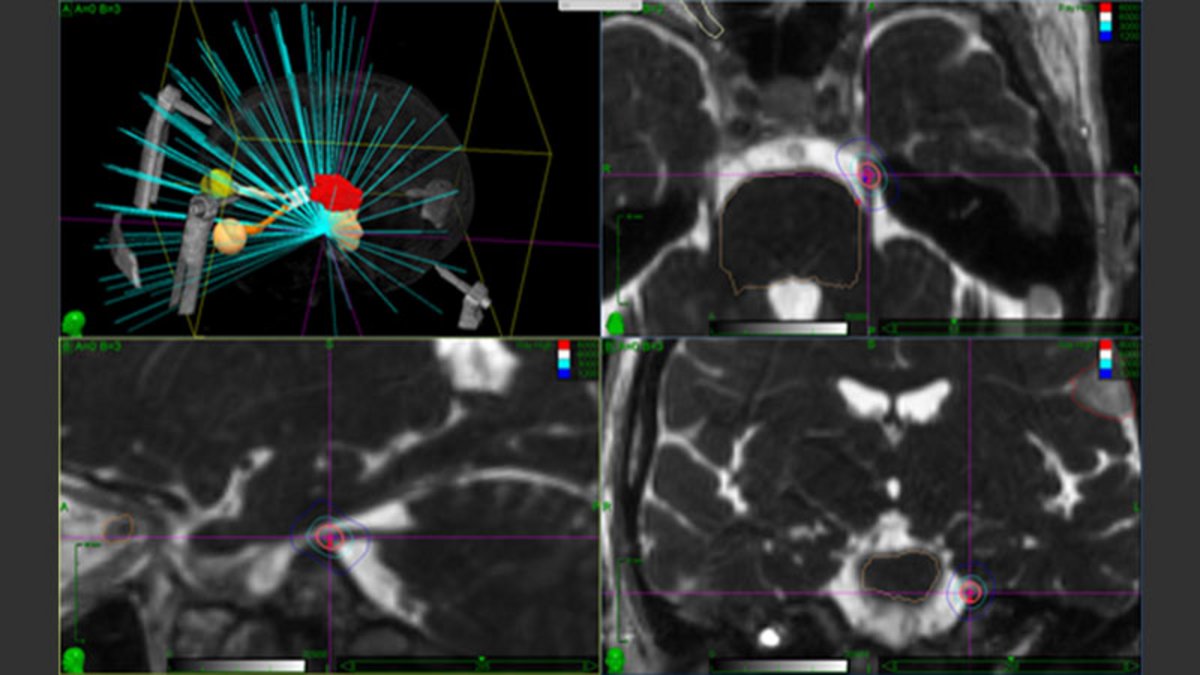
Stereotactic radiosurgery is a minimally invasive treatment method in which the trigeminal nerve is targeted with high-precision radiation. The procedure is performed on an outpatient basis and typically in a single session.
Using the CyberKnife or a Gamma Knife, the nerve is irradiated with millimeter precision just before it enters the brainstem. Over the course of several weeks, the radiation causes a targeted change in the nerve, which can thereby reduce the transmission of pain signals.
Radiosurgery is used in particular for patients for whom other treatment methods are not possible, are not sufficiently effective, or whose symptoms have recurred after previous treatment.
What are the success rates of these surgeries?
Overall, the prospects for success with the various treatment methods are very good. However, the results vary depending on the method, the initial condition, and the duration of follow-up.
Jannetta microvascular decompression
Following microvascular decompression, over 90% of patients report a significant reduction in pain or complete freedom from pain immediately after the procedure. For a large proportion of patients, this improvement is long-lasting; approximately 70% remain pain-free even after 10 years. Serious complications are rare and occur in about 1% of procedures.
Balloon Compression
Balloon compression leads to a significant reduction in pain in about 70–90% of patients. Compared to microvascular decompression, however, the likelihood of pain recurrence is higher *.
Stereotactic radiosurgery
Stereotactic radiosurgery can achieve significant pain relief in a large proportion of patients. Pain-free status is reported in up to 76% of cases and persists for over three years in about 60% of those treated. The most common side effect is changes in facial sensation *.
Your treatment at Inselspital
At Inselspital, the appropriate treatment is determined on an individual basis based on the neurological examination and MRI findings. During a detailed consultation, the various treatment options are discussed, and the therapy best suited to your specific situation is selected together.
We offer the full range of treatment options for trigeminal neuralgia:
Following a procedure, regular follow-up visits are scheduled, including a repeat neurological examination and an assessment of the treatment’s success. If pain is significantly reduced, medication can often be gradually reduced and tapered off. If the desired effect is not achieved, further treatment options can be explored.
-
Berger I, Nayak N, Schuster J, Lee J, Stein S, Malhotra NR. Microvascular Decompression Versus Stereotactic Radiosurgery for Trigeminal Neuralgia: A Decision Analysis. Cureus. 2017;9(1):e1000.
-
Chin L, Regine WF. Principles and Practice of Stereotactic Radiosurgery. 2nd Edition. Springer-Verlag New-York. 2015.