A herniated disc in the lumbar spine is the most common type of herniated disc. In this condition, disc tissue can press on nerves and cause sciatic pain that radiates from the buttocks down the leg to the foot. In most cases, symptoms improve with conservative treatment within a few weeks. Only if symptoms persist or neurological deficits occur is microsurgical surgery necessary, which provides rapid relief in about 95% of patients.
What is a herniated disc?
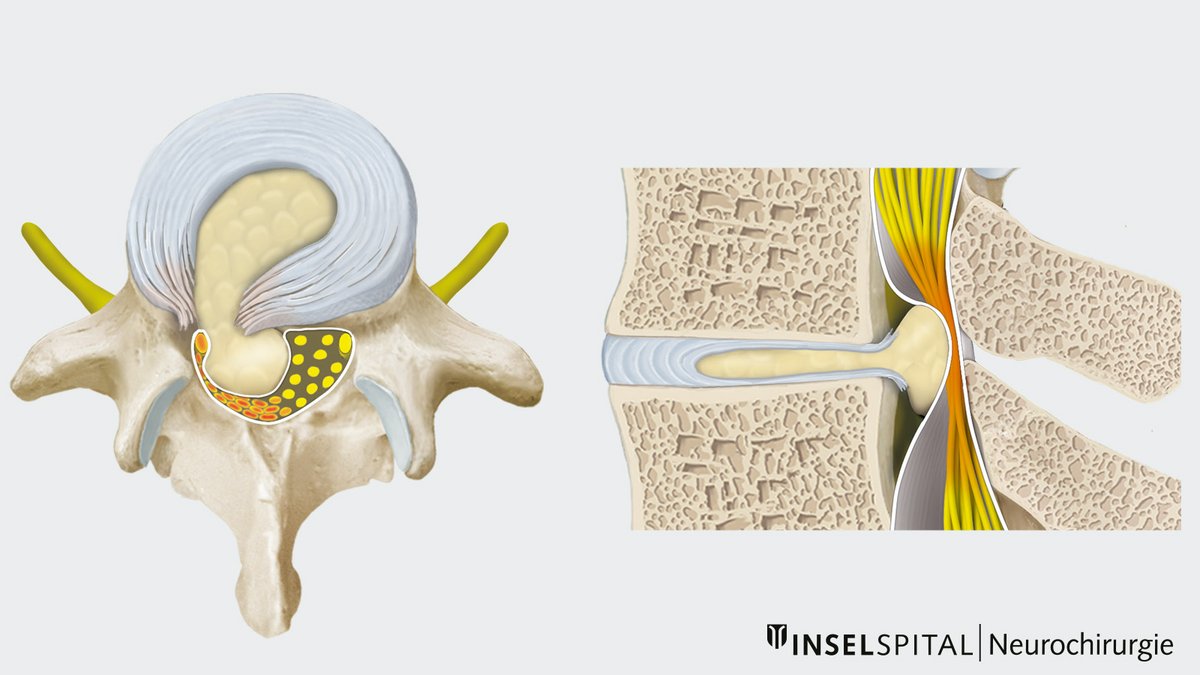
A herniated disc involves tears in the outer fibrous ring of the disc (annulus fibrosus). As a result, parts of the soft disc nucleus (nucleus pulposus) can protrude into the spinal canal. This tissue can compress nerves or the spinal cord and cause corresponding symptoms.
Since the body has no natural repair mechanisms in the intervertebral disc space, advanced degeneration cannot heal completely on its own.
Common – but rarely requiring surgery
Disc problems in the lumbar spine are common, but rarely require surgery. More than 90% of disc bulges or herniations with pain radiating into the leg improve with conservative treatment. This includes:
- Rest and heat
- Pain medication
- Relieving positioning
- Physical therapy
- Targeted injections
Distinction from «lumbago»
It is important to distinguish this from simple back pain (lumbalgia). This is usually caused by irritation of the vertebral joints or ligamentous structures and does not cause pain in the leg.
In these cases, rest is less important. On the contrary: movement is a central component of therapy and supports a faster recovery.
Patience often pays off
Whenever possible, we recommend conservative treatment for 6–12 weeks for a herniated disc. Symptoms often do not improve significantly until the second half of this period. It is therefore worthwhile to continue treatment consistently.
What is the cause of a herniated disc?
A herniated disc is the result of aging and wear and tear of the spine, which begins as early as the age of 20. The incidence of the disease increases continuously up to the age of 45 and then slightly decreases again. 2–3% of the population will experience a lumbar disc herniation that causes symptoms at some point in their lives.
Heavy physical work, incorrect strain and genetic factors favor these processes and degenerative changes.
Additional risk factors such as smoking also play an important role.
What are the most common symptoms of a lumbar disc herniation?
Disc herniations most commonly occur between the 4th and 5th lumbar vertebrae (L4/L5) and between the 5th lumbar vertebra and the sacrum (L5/S1). These areas are subject to the greatest mechanical stress on the intervertebral discs.
Depending on the direction in which the disc material bulges or herniates, either the protruding nerve root or the nerve root running beneath it in the spinal canal may be affected. Pressure on the nerves causes irritation or functional disorders.
Typical symptoms include:
- Radiating pain from the lower back through the buttocks and leg down to the foot (sciatica)
- Sensory disturbances such as tingling or numbness
- Muscle weakness or paralysis in the affected leg
- Additionally, back pain in the lumbar spine area is common (lumbar sciatica)
Since each nerve root supplies a specific skin area (dermatome) and muscle area (myotome), the symptoms often allow for a relatively precise identification of the affected nerve root.

Locating the incident based on symptoms
Typical symptoms associated with the nerve root are:
- L4: Pain in the thigh extending down to the knee, numbness in the front of the thigh and the inner side of the lower leg, lack of strength when climbing stairs (knee extensors).
- L5: Pain in the buttocks and along the outer edge of the thigh down to the foot, numbness in the big toe, weakness of the foot extensor muscles, particularly the big toe extensor (standing on heels).
- S1: Pain in the buttocks and the back of the leg extending to the foot, numbness along the outer edge of the foot and in the little toe, weakness of the plantar flexor (toe stand).
This list is not exhaustive.
A rare but serious complication: cauda equina syndrome
In cases of very large herniated discs, multiple nerve roots can become compressed simultaneously within the spinal canal. This condition is known as cauda equina syndrome.
Typical warning signs may include:
- Bladder or bowel dysfunction
- Numbness in the buttocks or genital region
- Weakness in both legs
Cauda equina syndrome is a neurosurgical emergency. Once confirmed by imaging, surgery must be performed promptly to prevent permanent nerve damage and lasting functional deficits as much as possible.
How is a lumbar disc herniation diagnosed?
A detailed medical history and thorough clinical examination are crucial for the initial evaluation of symptoms involving the lumbar spine. If back pain occurs without any other symptoms, imaging studies may not be necessary at first. In most cases, conservative treatment is sufficient, as symptoms often improve within a few weeks.
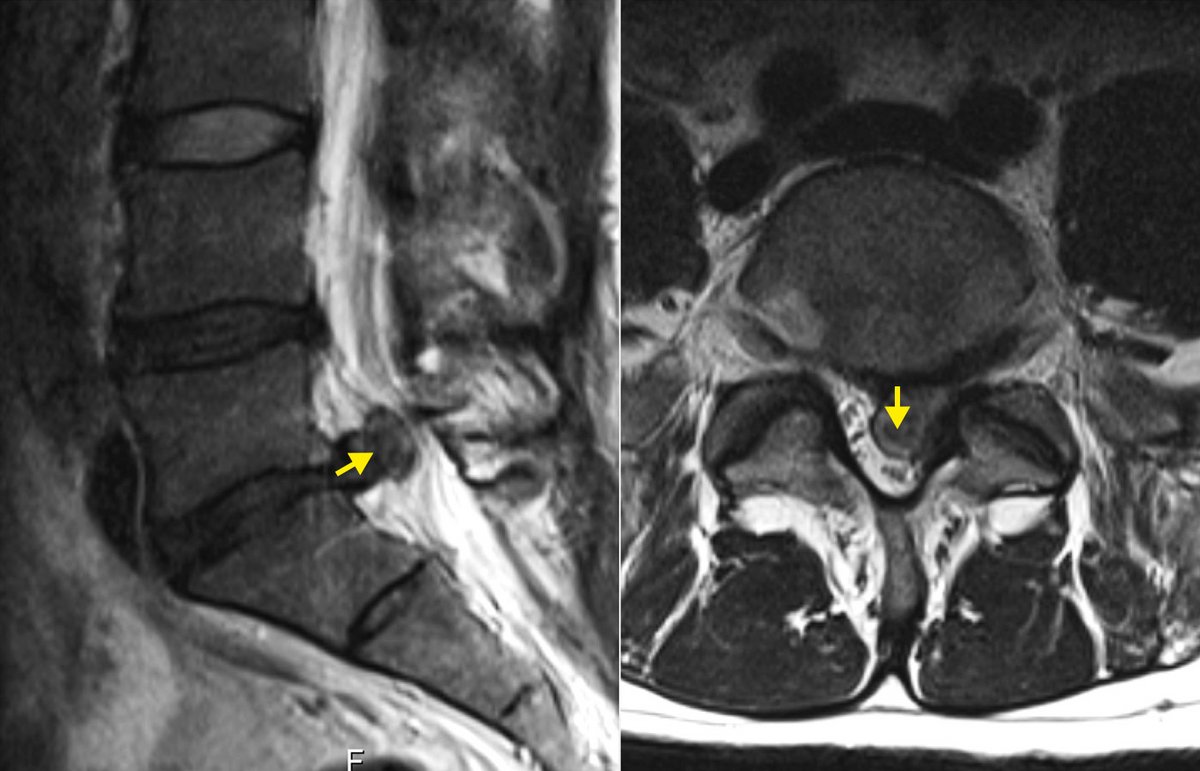
However, if the pain persists or neurological deficits occur, imaging studies are necessary. Magnetic resonance imaging (MRI) is the method of choice for this purpose, as it is particularly effective at visualizing intervertebral discs and nerve roots.
Only in rare special cases are additional examinations such as electrophysiological tests or a CT myelography necessary.
What does the surgical procedure involve?
Surgery is recommended if the pain is very severe, muscle weakness develops, or conservative treatment does not provide sufficient relief.
The procedure typically lasts 15–45 minutes and is performed through a small incision of about 2–3 cm. Access to the intervertebral disc is usually achieved via a special tube (tubular access). The surgery is performed using microsurgical techniques under an operating microscope. This technique allows for a precise and tissue-sparing procedure with a small incision and a clear view of the affected nerve structures.
After the surgery, you will receive early care from our physical therapists. In addition, you will receive a brochure with exercises and recommendations for the period following your discharge.
The hospital stay is usually 2–3 days. In select cases, the procedure can also be performed on an outpatient basis.

Prospects of the surgery
Microsurgical removal of a herniated disc is the most common surgical procedure performed on the lumbar spine and has been an established neurosurgical technique for many years.
In approximately 95% of patients, symptoms improve rapidly. However, in 5–20% of cases, a recurrent disc herniation may occur if disc tissue protrudes into the spinal canal again. The risk depends primarily on the size of the tear in the annulus fibrosus of the disc and less on whether the initial treatment was conservative or surgical.
Should a recurrence occur, further treatment will be discussed on an individual basis. Options range from another minimally invasive microsurgical procedure to stabilization procedures such as spinal fusion, particularly in cases of repeated recurrences.
Our experience at Inselspital
At the Inselspital Spine Center, specialists from various disciplines work closely together. These include neurosurgery, orthopedics, neurology, rheumatology, neuroradiology, physical therapy, and the Pain Center.
This interdisciplinary collaboration allows us to develop a personalized treatment strategy for each patient. Complex cases are discussed in an interdisciplinary board and, if necessary, operated on jointly by neurosurgeons and orthopedic surgeons.
The minimally invasive microsurgical removal of a herniated disc to relieve pressure on a pinched nerve is one of the most common procedures at our clinic and, in selected cases, can also be performed on an outpatient basis.
Studies show that surgery for persistent symptoms after 6–12 weeks of conservative treatment can often lead to faster improvement *, *. Nevertheless, the following applies: Most herniated discs can be treated without surgery.
Our nurses and physical therapists have extensive experience in caring for patients following a herniated disc. They support patients while they are still in the hospital and prepare them for the recovery period.
Since proper behavior in daily life plays an important role in recovery, we provide our patients with informational materials, including:
- Tips on proper lifting and carrying
- Back exercises
- A video with recommendations for the post-operative period
-
Lurie JD, Tosteson TD, Tosteson AN et al. Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for the spine patient outcomes research trial. Spine (Phila Pa 1976). 2014;39:3-16.
-
Bailey CS, Rasoulinejad P, Taylor D et al. Surgery versus Conservative Care for Persistent Sciatica Lasting 4 to 12 Months. N Engl J Med. 2020;382:1093-1102.
Further reading
- Weinstein JN, Lurie JD, Tosteson TD et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT) observational cohort. JAMA. 2006;296:2451-2459.
- Vialle LR, Vialle EN, Suárez Henao JE, Giraldo G. LUMBAR DISC HERNIATION. Rev Bras Ortop. 2010;45:17-22.
- Heindel P, Tuchman A, Hsieh PC et al. Reoperation Rates After Single-level Lumbar Discectomy. Spine (Phila Pa 1976). 2017;42:E496-E501.