Lymphomas are malignant tumors of the lymphatic system that can also affect the brain or spinal cord. A tissue sample is taken to confirm the diagnosis. Treatment typically consists of a combination of immunotherapy and chemotherapy and is tailored to the specific type of the disease.
How common are lymphomas of the central nervous system?
Generally, there are two types of central nervous system (CNS) lymphoma:
- Primary CNS lymphoma (PCNSL): This originates directly in the brain, the meninges, the eyes, or the spinal cord and remains confined to the central nervous system.
- Secondary CNS lymphoma: This involves metastases of a lymphoma that originally developed in other organs. Typically, this involves tumors of the hematopoietic organs, which first affect the lymph nodes or the spleen and only later spread to the central nervous system.
Primary CNS lymphomaaccounts for about 4% of all primary tumors of the central nervous system. It primarily affects older patients aged 65 to 85, with the highest incidence among those over 75. The annual incidence is approximately 0.4 per 100,000 people, but rises to about 4 per 100,000 among those over 70.
In secondary CNS lymphoma, the central nervous system is affected in the course of an already existing systemic lymphoma. This includes, for example, non-Hodgkin lymphoma (NHL), which initially developed in the lymph nodes or the spleen. The frequency with which the CNS is affected varies depending on the type of lymphoma and ranges from about 3% to 50%. In most patients with systemic lymphoma (non-Hodgkin lymphoma, NHL), the central nervous system is not affected at the time of initial diagnosis.
In general, the incidence of lymphomas has increased in recent decades compared to other brain lesions. Those most commonly affected are patients with a compromised immune system, such as those undergoing immunosuppressive therapy for cancer, following organ transplants, or with AIDS.
What are the causes of lymphoma?
Lymphomas are tumors that arise from abnormal cells of the hematopoietic system. In over 90% of cases, primary central nervous system lymphoma (PCNSL) is a specific, rapidly growing form of lymphoma that originates from malfunctioning immune cells.
The exact causes of PCNSL are largely unknown. However, it is believed that the immune system plays an important role, as PCNSL typically does not occur throughout the entire body (systemically). Additionally, in immunocompromised patients, there is a possible link to the Epstein-Barr virus (EBV), although this virus is not detectable in all affected individuals.
The most important risk factor is immunodeficiency. This can result from:
- immunosuppressive therapies following an organ transplant
- HIV infection
- congenital immunodeficiencies
Certain inflammatory or autoimmune diseases are also associated with an increased risk, including:
- systemic lupus erythematosus
- rheumatoid arthritis
- vasculitides (inflammatory vascular diseases)
In secondary CNS lymphomas, the tumor cells reach the central nervous system either via the bloodstream or through direct spread from the adjacent bone marrow.
What symptoms does CNS lymphoma cause?
In most cases (>50%), central nervous system (CNS) lymphomas initially present with nonspecific symptoms such as personality changes or mood swings, as well as signs of increased intracranial pressure (headaches, fatigue, nausea, and vomiting).
About 10% of patients experience epileptic seizures.
In about one-third of those affected, so-called focal neurological deficits also occur. These include, for example:
- Hemiparesis
- Impaired cranial nerve functions (e.g., double vision or taste and smell impairments)
How is lymphoma diagnosed?
Using imaging techniques such as computed tomography (CT) and magnetic resonance imaging (MRI), lymphomas are often difficult to distinguish from other tumors of the nervous system. This is where modern neurosurgery can play a key role.
Lumbar Puncture
If radiological findings suggest a CNS lymphoma, a lumbar puncture may be performed as a first step. During this procedure, cerebrospinal fluid (CSF) is withdrawn from the spinal canal and examined. Using molecular genetic testing (Next-Generation Sequencing, NGS), certain tumor markers can be detected, such as MYD88 or interleukin-10. These findings can indicate primary CNS lymphoma (PCNL) with a high degree of accuracy.
In selected cases, this test may be sufficient on its own, making a brain biopsy unnecessary.
Biopsy
A tissue sample followed by histopathological examination is still considered an essential step in establishing a definitive diagnosis and planning further treatment. Discuss with our specialists which procedure is most suitable for you:
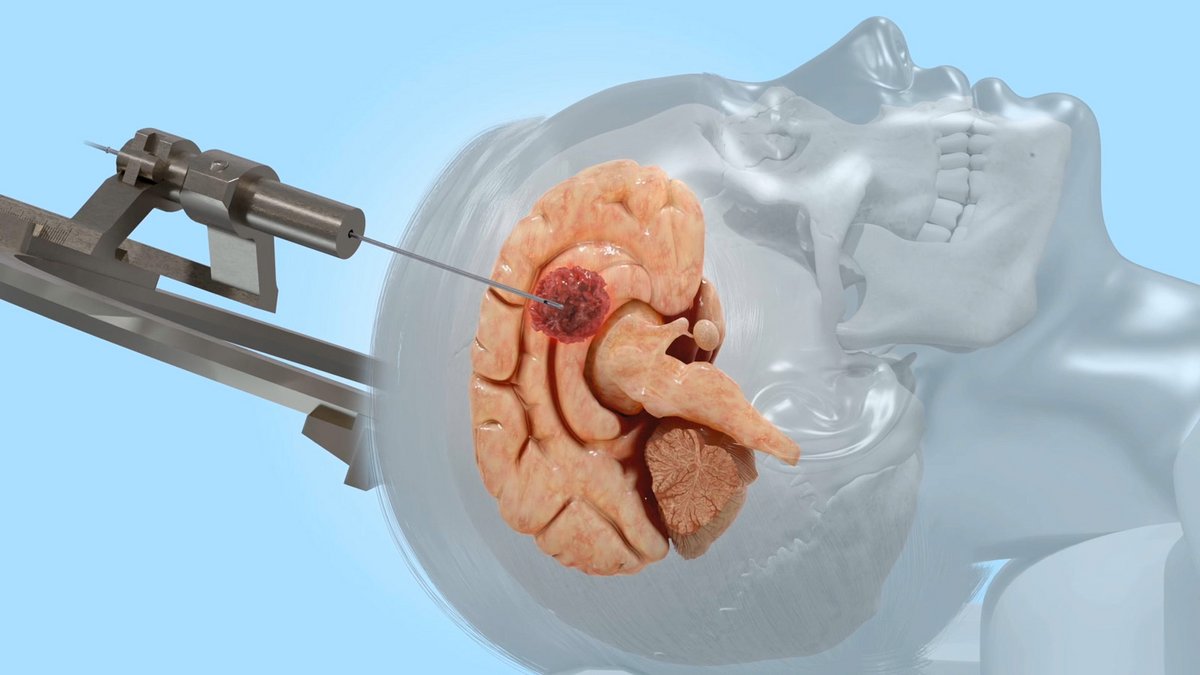
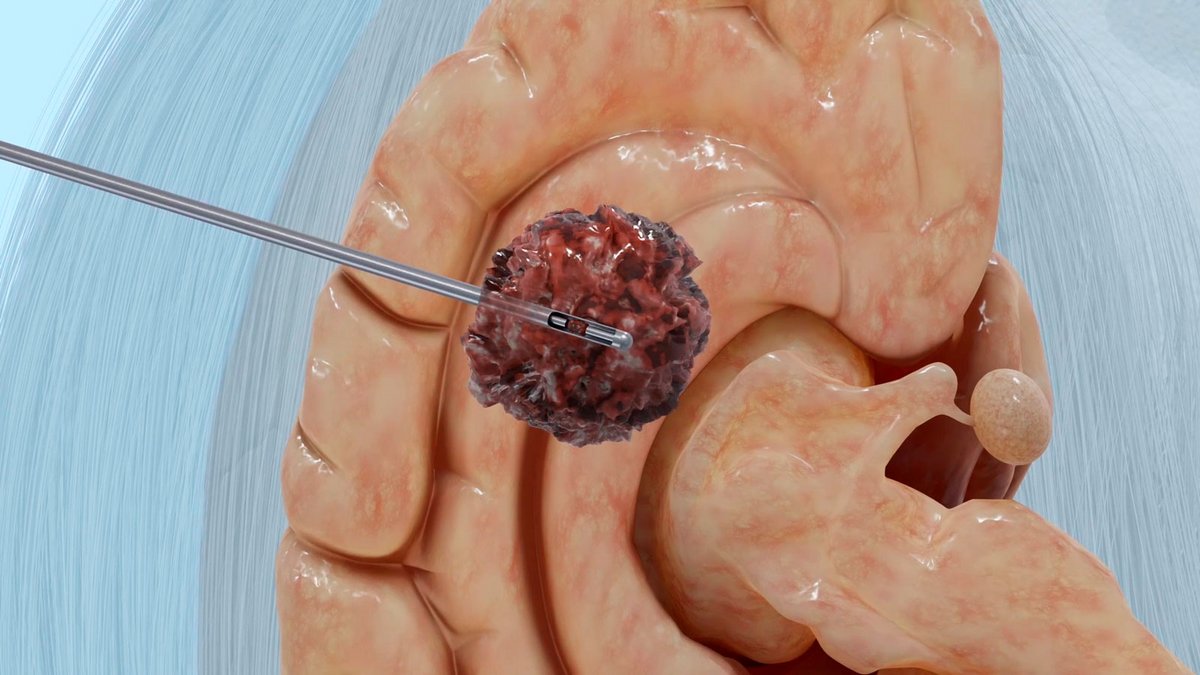
- Stereotactic biopsy is an elegant, minimally invasive neurosurgical procedure for the gentle and millimeter-precise removal of brain tissue.
- Alternatively, another image-guided, computer-assisted 3D navigation procedure can be used for precise tissue sampling: the so-called VarioGuide.
- In the case of superficial involvement, tissue sampling can also be performed as part of a small craniotomy under direct visualization (open biopsy).
Stereotactic biopsy is one of the safest and most effective methods for diagnosing CNS lymphomas. The most common complication is cerebral hemorrhage, which occurs in rare cases (<1%). With open biopsy, the risk of complications such as bleeding or infection is slightly higher due to the procedure’s greater invasiveness.
In rare cases, the histological examination following a biopsy does not yield a clear result, so a repeat procedure may be necessary.
The histopathological examination and molecular typing of the tumor tissue following a biopsy are performed in the Department of Neuropathology. These provide clarity regarding the exact diagnosis. In this way, a lymphoma can be clearly distinguished from other brain tumors.
Systemic diagnostics
A comprehensive diagnostic workup also includes a systemic tumor search. This involves using computed tomography (CT) to specifically search for tumors in areas where lymphomas typically develop. These include the lymph node regions in the neck, chest, groin, and pelvis.
A nuclear medicine examination using FDG-PET/CT, particularly to investigate a suspected secondary CNS lymphoma, is also part of the diagnostic workup.
How is lymphoma treated?
Unlike other tumors of the nervous system, lymphoma generally cannot be surgically removed. Surgical removal (resection) does not improve survival rates in cases of lymphoma. Therefore, stereotactic biopsy to confirm the diagnosis and subsequent drug therapy constitute the standard of care.
After the lymphoma has been precisely characterized, induction therapy is first administered using highly effective chemotherapeutic agents (often methotrexate, sometimes in combination with rituximab). This is typically followed by consolidation therapy using high-dose chemotherapy.
For therapy-resistant (refractory) lymphomas, immunotherapies or CAR-T cell therapies may be considered in selected cases.
Brain radiation may be considered in certain situations, but is no longer part of the standard treatment for CNS lymphomas.
Why you should seek treatment at Inselspital
At the Inselspital Neurocenter, the planning and implementation of optimal treatment are carried out by a multidisciplinary team of specialists in neurosurgery, neuroradiology, neuropathology, oncology, and radiation oncology, who have extensive experience in the diagnosis and treatment of this condition.
This interdisciplinary team meets weekly as part of a lymphoma board and determines the best possible treatment strategy for each patient on an individual basis.
Further reading
- Chukwueke UN1, Nayak L2. Central Nervous System Lymphoma. Hematol Oncol Clin North Am. 2019 Aug;33(4):597-611.
- Gleissner B, Chamberlain M. Treatment of CNS dissemination in systemic lymphoma. J Neurooncol. 2007 Aug;84(1):107-17.
- Greenberg M. Handbook of Neurosurgery. Eight Edition. Thieme Medical Publishers Inc; 2016
- Hoffman S, et al. Temporal trends in incidence of primary brain tumors in the United States, 1985-1999. Neuro Oncol. 2006 Jan;8(1):27-37.
- Keldsen N, et al. Risk factors for central nervous system involvement in non-Hodgkins-lymphoma--a multivariate analysis. Acta Oncol. 1996;35(6):703-8.
- O'Neill BP, Illig JJ. Primary Central Nervous System Lymphoma. Mayo Clin Proc. 1989 Aug;64(8):1005-20.
- Rubenstein JL, et al. Intensive chemotherapy and immunotherapy in patients with newly diagnosed primary CNS lymphoma: CALGB 50202 (Alliance 50202). J Clin Oncol. 2013 Sep 1;31(25):3061-8.
- Yoshida S, et al. Characteristic features of malignant lymphoma with central nervous system involvement. Surg Neurol. 2000 Feb;53(2):163-7.