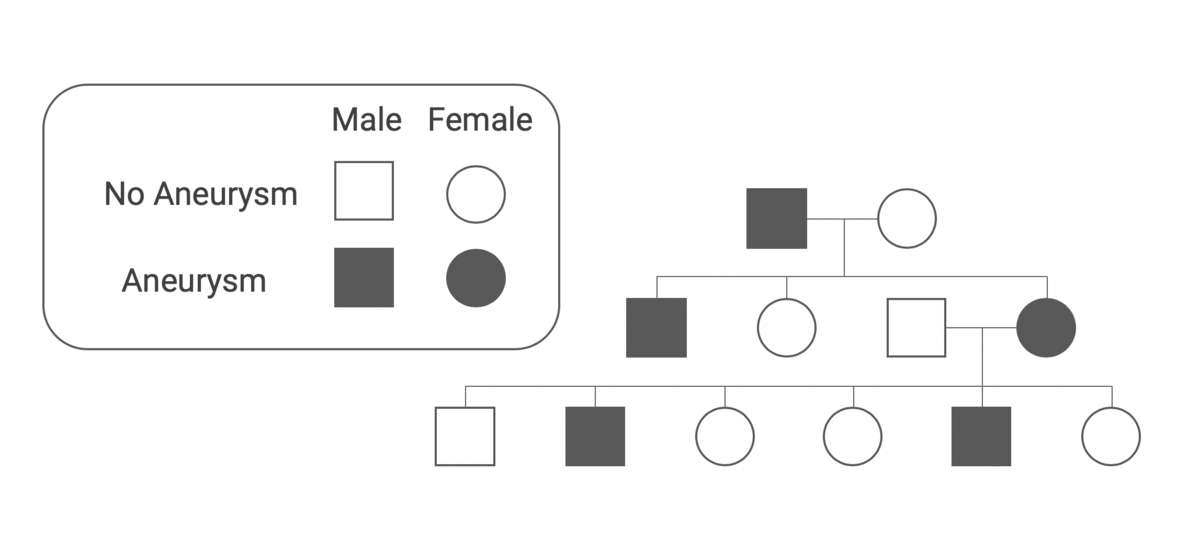
In rare cases, cerebral artery aneurysms can run in families. If two or more close first-degree relatives are affected, this is referred to as familial clustering. In this case, the risk for other family members is increased. Therefore, preventive imaging examinations are recommended in cases of familial clustering of aneurysms.
Special aneurysm consultation at the Inselspital
During our aneurysm consultation with Prof. Andreas Raabe and Prof. David Bervini, you will receive comprehensive and personalized advice. We will answer all your questions about the causes, heredity, risks, and treatment options for cerebral artery aneurysms.
Frequent topics include:
- Can an aneurysm be inherited?
- When is screening advisable for family members?
- Is aneurysm screening recommended if only one family member has an aneurysm?
- What are the advantages and limitations of screening?
We are happy to take the time to discuss your individual situation during our special consultation hours. You can be referred by your doctor or contact us directly.
Can an aneurysm be inherited?
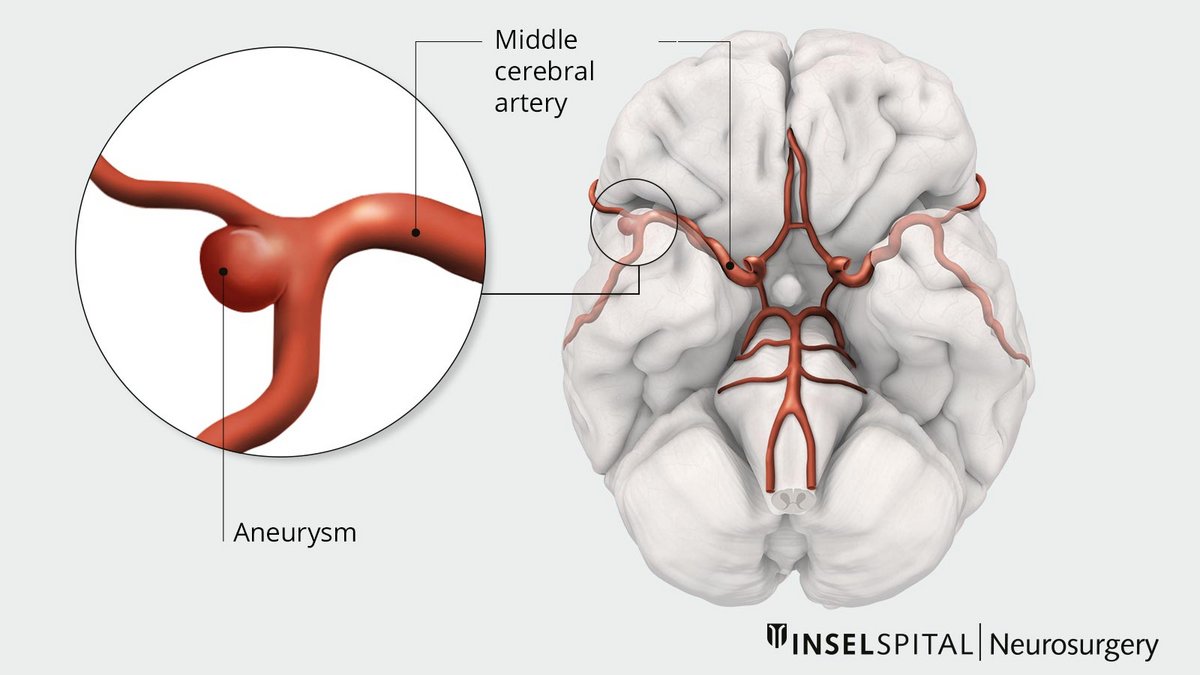
Aneurysms of the cerebral arteries are often incidental findings and usually remain harmless. However, they can also rupture and cause dangerous cerebral hemorrhaging. This raises the question for patients' relatives: Are aneurysms hereditary? The answer is yes—but this only applies to a small proportion of aneurysms.
Familial clustering and aneurysm risk
- In the general population, the prevalence of an aneurysm is about 2%.
- If a first-degree relative (parent, sibling, or child) has an aneurysm, the risk increases to about 4%.
- If two first-degree relatives are affected, the risk increases to about 8%. This risk may rise further in the presence of additional risk factors such as hypertension or active smoking.
- The lifetime risk of suffering a subarachnoid hemorrhage due to an aneurysm rupture is estimated at about 26 % if two first-degree relatives have a history of ruptured intracranial aneurysms. *
Familial polycystic kidney disease and aneurysm risk
Certain diseases such as familial cystic kidneys are also associated with an increased risk:
- Approximately 12% of those affected also have an intracranial aneurysm.
- The risk of an aneurysmal subarachnoid hemorrhage is up to 25 times higher than in the general population.
- Evidence from studies suggests that second- and third-degree relatives may also have a slightly increased risk.
When is screening advisable for family members?
A familial aneurysm disease is diagnosed when two or more first-degree relatives suffer from an aneurysm. If desired, these relatives can be specifically screened for aneurysms using a non-invasive examination such as magnetic resonance angiography (MRA).
In affected families, aneurysms not only occur more frequently, but the overall risk is also increased. Familial aneurysms are associated with a higher risk of rupture. In the event of a rupture, family members are also usually younger and have a higher mortality rate. *
In the case of identical twins, if an aneurysm has been detected in one twin, it is advisable to examine the other twin as well. The same applies to patients with autosomal dominant polycystic kidney disease.
A large study has found new evidence regarding the risk of rupture in familial aneurysms *. Aneurysms were diagnosed in 20.6% of the first-degree relatives examined. All belonged to a risk group – they smoked or had high blood pressure. The risk of rupture was around 1.2% per year, even for small aneurysms (<7 mm) in the anterior circulation.
We recommend that young people from families in which at least two first-degree relatives have an aneurysm undergo a preventive examination using MR angiography without contrast medium every 5–7 years from the age of 20. However, this is conditional on the individuals concerned themselves wishing to undergo the examination.
This recommendation is based on a study by Dutch researchers at Utrecht University *. The study showed that screenings conducted every 5–10 years detected a new aneurysm in 5% of participants, even if previous examinations had been negative.
Is aneurysm screening recommended if only one family member has an aneurysm?
If an aneurysm is present in only one first-degree relative, no screening is generally recommended for other family members. In this group, the prevalence of aneurysms in Central Europe is not significantly higher than in the general population. The aneurysms detected are usually small and located in the anterior circulation, so the risks of treatment currently outweigh the potential benefits *.
What are the benefits and limitations of screening?
The decision on whether to specifically screen for a previously undetected brain aneurysm is made by the patient in consultation with an aneurysm specialist. A clear desire to undergo screening is a prerequisite, as a magnetic resonance imaging (MRI) scan of the head may also reveal other incidental findings.
Before the examination, potential consequences and complications of treatment, insurance-related issues, suitability for certain activities, and the risk of findings that cannot be treated should be discussed. Simply knowing about an aneurysm can be a psychological burden for those affected, even if there is no immediate need for medical intervention.
We are currently conducting a screening study for aneurysms in patients who have chronic nicotine use as a risk factor.
-
Raaymakers TW. Aneurysms in relatives of patients with subarachnoid hemorrhage: frequency and risk factors. MARS Study Group. Magnetic Resonance Angiography in Relatives of patients with Subarachnoid hemorrhage. Neurology. 1999;53:982-988.
-
Rinkel GJ. Intracranial aneurysm screening: indications and advice for practice. Lancet Neurol. 2005;4:122-128.
-
Broderick JP, Brown RD, Sauerbeck L et al. Greater rupture risk for familial as compared to sporadic unruptured intracranial aneurysms. Stroke. 2009;40:1952-1957.
-
Bor AS, Rinkel GJ, van Norden J, Wermer MJ. Long-term, serial screening for intracranial aneurysms in individuals with a family history of aneurysmal subarachnoid haemorrhage: a cohort study. Lancet Neurol. 2014;13:385-392.