The procedure of 5-ALA fluorescence is used at the Inselspital to make malignant tumor cells visible during surgery. Malignant tumors grow invasively and infiltratively, making it difficult for the surgeon to distinguish the edges of the tumor from the surrounding healthy brain tissue. When using 5-aminolevulinic acid, or shortly 5-ALA, a metabolic product of the tumor cell is illuminated by a special blue light. Tumor cells not visible to the naked eye can be detected and removed under this light.
How can malignant tumor cells be made visible?
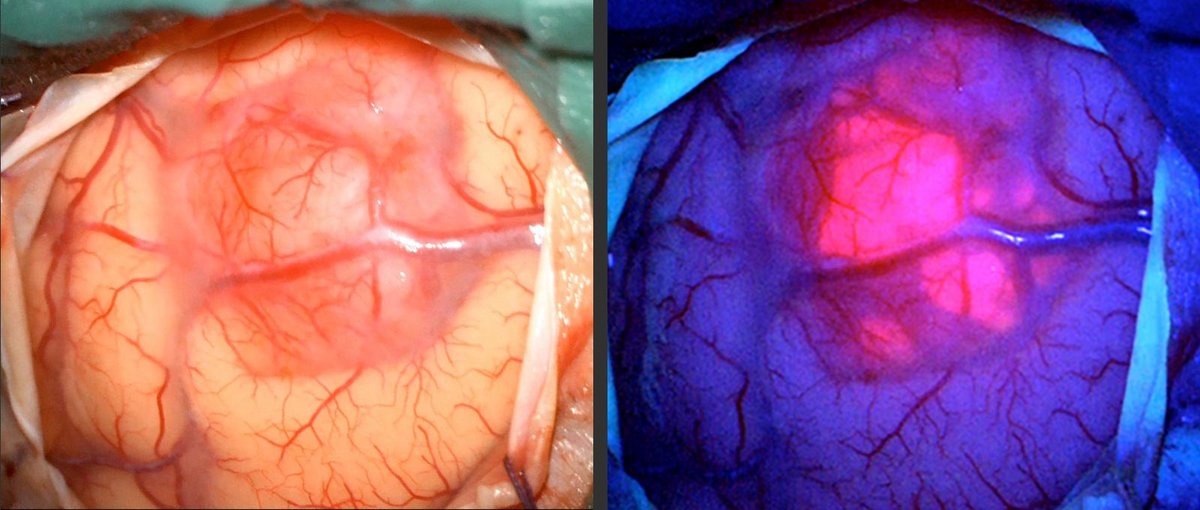
An important component of modern tumor surgery is the administration of 5-aminolevulinic acid (abbreviated as 5-ALA or Gliolan®), which is now routinely used. 5-ALA is an amino acid formed in the body (endogenous) that occurs as a metabolite in human heme metabolism, where it is converted to protoporphyrin IX. When protoporphyrin IX is illuminated with a special blue light, it produces a red fluorescence signal.
Now, the methodology of 5-ALA fluorescence imaging comes into play: Tumor cells have a different metabolism than normal brain cells and, due to an enzyme defect, cannot fully process certain amino acids. This leads to an accumulation of protoporphyrin IX in the tumor cells *. During surgery, a light signal with a wavelength of 440 nm can be emitted from the surgical microscope through a special filter, causing the accumulated protoporphyrin IX in the tumor cells to fluoresce in red color. This allows the tumor tissue to be clearly distinguished from the surrounding healthy brain tissue and subsequently surgically removed. Therefore, this procedure helps maximize the extent of resection and improve the surgical outcome *, *.
In other medical specialties such as urology, ophthalmology, and dermatology, this procedure has been used for some time. Now, it has gradually become the standard in the surgery of malignant brain tumors *.
The fluorescence signal observed intraoperatively can appear reddish or more pinkish. In a prospective study to evaluate the effectiveness of the methodology, 52 patients with glioblastoma participated. The study showed a correlation of the red signal with pronounced tumor tissue, which already exhibited vascular formations (neovascularization) in histopathology. In contrast, the pink fluorescence signal could be observed especially in the transition zone between tumor tissue and normal brain tissue *.
Benefits of 5-ALA fluorescence for surgery and prognosis in glioblastoma
The clinical benefit of using 5-ALA in neurosurgery was demonstrated in a controlled randomized study in 2006 *. This groundbreaking study showed that administration of 5-ALA resulted in a significantly higher rate of complete tumor resections. It also confirmed the effectiveness of surgical therapy: if the tumor could be completely removed, meaning no tumor residue was detectable on the day after the operation in the MRI, then the average survival time significantly increased.
For which patients is 5-ALA used?
5-ALA is routinely used in patients suspected of having a high-grade glioma (glioblastoma, astrocytoma). However, the pathological accumulation of 5-ALA is not limited to high-grade gliomas but can also occur, for example, in metastases or meningiomas. However, the evidence from current literature shows a clear clinical benefit only in high-grade gliomas *. Therefore, the application of 5-ALA in other tumor diseases is only performed in specific cases.
Depending on the location of the tumor, we combine 5-ALA fluorescence with electrophysiological methods for intraoperative functional monitoring to achieve the most radical tumor resection with maximum patient safety.
In one of our studies, we demonstrated that more tumor tissue can be removed with 5-ALA than could be visualized in an MRI image before the operation. This means that 5-ALA is more sensitive for the visualization of tumor cells than MRI. Therefore, consistent use of 5-ALA can achieve a more radical resection in high-grade gliomas *.
What are the side effects of using 5-ALA?
In 2007, 5-ALA received approval from the European Medicines Agency (EMA) for intraoperative use in malignant gliomas under the trade name Gliolan®.
Common side effects following the administration of 5-ALA include laboratory changes in blood counts such as anemia, thrombocytopenia, or leukocytosis, as well as elevated liver enzymes. Depending on the severity, these side effects may need to be further monitored with laboratory tests.
Patients with an enzyme defect in porphyrin metabolism (porphyria) are advised against the use of 5-ALA. Similarly, there is a contraindication for the use of 5-ALA during pregnancy.
5-ALA is considered a potentially phototoxic substance. This means that patients should avoid exposure to strong light sources for 24 hours after ingestion. This includes direct sunlight, bright and intense indoor lighting, as well as operating room lighting. Concurrent administration of other potentially phototoxic substances (e.g., tetracyclines, sulfonamides, fluoroquinolones, hypericin extracts) should be avoided.
-
Hefti M, von Campe G, Moschopulos M, Siegner A, Looser H, Landolt H. 5-aminolevulinic acid induced protoporphyrin IX fluorescence in high-grade glioma surgery: a one-year experience at a single institutuion. Swiss Med Wkly. 22. März 2008;138(11–12):180–5.
-
Hadjipanayis CG, Widhalm G, Stummer W. What is the Surgical Benefit of Utilizing 5-ALA for Fluorescence-Guided Surgery of Malignant Gliomas? Neurosurgery. November 2015;77(5):663–73.
-
Stummer W, Reulen H-J, Meinel T, Pichlmeier U, Schumacher W, Tonn J-C, et. al. Extent of resection and survival in glioblastoma multiforme: identification of and adjustment for bias. Neurosurgery. März 2008;62(3):564–76;
-
Stummer W, Pichlmeier U, Meinel T, Wiestler OD, Zanella F, Reulen H-J, et. al. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial. Lancet Oncol. Mai 2006;7(5):392–401.
-
Stummer W, Novotny A, Stepp H, Goetz C, Bise K, Reulen HJ. Fluorescence-guided resection of glioblastoma multiforme by using 5-aminolevulinic acid-induced porphyrins: a prospective study in 52 consecutive patients. J Neurosurg. Dezember 2000;93(6):1003–13.
-
Ferraro N, Barbarite E, Albert TR, Berchmans E, Shah AH, Bregy A, et. al. The role of 5-aminolevulinic acid in brain tumor surgery: a systematic review. Neurosurg Rev. Oktober 2016;39(4):545–55.
-
Schucht P, Knittel S, Slotboom J, Seidel K, Murek M, Jilch A, et. al. 5-ALA complete resections go beyond MR contrast enhancement: shift corrected volumetric analysis of the extent of resection in surgery for glioblastoma. Acta Neurochir (Wien). Februar 2014;156(2):305–12;