Fiber tracking is a specialized analysis of MRI images that makes it possible to visualize key nerve fiber tracts in the brain. These tracts connect different regions of the brain and are responsible for functions such as movement, speech, and vision. Before neurosurgical procedures, fiber tracking helps map the exact course of these delicate structures. This allows surgeries to be planned more precisely and helps better protect important brain functions.
What exactly is fiber tracking?
Fiber tracking is a specialized analysis of MRI images of the brain. This method allows us to visualize important nerve fiber tracts. These tracts connect different areas of the brain and are responsible, for example, for movement, speech, or vision.
In certain conditions, such as brain tumors, these important connections may run near the affected region. Fiber tracking helps us map the exact course of these nerve tracts.
How does fiber tracking work?
Fiber tracking is based on a specialized MRI technique known as diffusion imaging. This technique measures how water molecules move within brain tissue. Within nerve fibers, water tends to move along the direction of the fibers. This property makes it possible to mathematically determine the course of fiber tracts and visualize them.
Using specialized software, this data is used to create three-dimensional representations of the nerve tracts.
Limitations of the method
Fiber tracking visualizes bundles of nerve fibers, not individual nerves, because the resolution of the underlying magnetic resonance imaging is limited. Furthermore, the visualization is based on mathematical models and can be influenced by various factors.
Despite modern imaging techniques such as high-definition fiber tracking, unexpected breaks in the reconstructed fibers still occur at intersection points and in areas where fibers change direction in a confined space. Identifying the relevant fibers, verifying their plausibility, and preparing them for use in surgical planning is a challenging task that requires a specialist.
Despite these limitations, the method provides important additional information and is today a valuable tool in modern neurosurgical planning.
How is fiber tracking used at Inselspital?
This technique is primarily used for planning neurosurgical procedures.
When a brain tumor or other lesion is located near important nerve pathways, it is crucial to know where these pathways run. Fiber tracking helps our neurosurgeons:
- identify important nerve pathways
- plan the best possible surgical approach
- reduce the risk of functional deficits
The information obtained can be integrated into surgical planning and navigation during the operation.
The goal is to achieve radical removal even of tumors in important functional areas of the brain. Together with intraoperative neurophysiology techniques, we thus achieve for our patients maximum radicality with minimal invasiveness and significant preservation of function.
To make surgeries even safer for patients in the future, research and development of innovative techniques such as fiber tracking constitute a distinct research focus here at Inselspital.
Fiber tracking in clinical application
- Planning of the fiber tracks
If an operation is to be performed with the aid of fiber tracking, the specially required DTI sequences and T2-weighted image sequences are created and merged in advance in a 3 Tesla magnetic resonance imaging (MRI). Using an automatic algorithm, artifacts (eddy current artifacts and motion artifacts) are automatically eliminated. To calculate the desired fiber bundles, a region of interest (ROI) is now superimposed over the relevant anatomical landmarks in the T2-weighted MRI imaging. Furthermore, one selects the parameters for fractional anisotropy and fiber bundle length.
For example, to calculate the pyramidal tract, the regions of interest are plotted along with the imaging anatomical landmarks of the pyramidal tract on the T2-weighted images: gyrus precentralis, capsula interna, and parts of the pedunculus cerebri. With the correctly chosen adjustment parameters, a homogeneous fiber bundle is obtained, which represents the course of the pyramidal tract.
")
Regions of interest (ROI). In T2-weighted MRI images, the ROIs are marked to calculate the pyramidal tract. The pyramidal tract (corticospinal tract) originates in the precentral gyrus (left image) and runs via the cerebral crus (right image) into the spinal cord. Bild: Nowacki et. al. 2018, JNS - Fiber tracking in tumor surgery
If a tumor is located near a vital fiber bundle, fiber tracking is necessary to ensure maximum patient safety. Often, the boundaries between healthy brain tissue and tumor tissue cannot be clearly delineated. The exact course of the fiber bundles in relation to the tumor provides the surgeon with important additional information that is not visible to the naked eye.
Together with other techniques such as intraoperative neuromonitoring, the surgeon has several options to ensure that no critical structures are injured during surgery. In particularbfiber connections which are necessary for basic human functions such as speech, vision, and movement are protected with great effort from unintended damage during tumor surgery.

Tumor surgery. (Left) The tumor to be removed (T) is in close proximity to the arcuate fasciculus (AF). The middle image shows the so-called voxels of interest (VOI), which were used to calculate the fiber bundle. On the right is the course of the arcuate fasciculus with Broca's center (B) and Wernicke's area (W) at each end of the fiber bundle. Bild: Stieglitz et. al. 2012, Neurosurgery 
Eloquent areas. This image shows a tumor (orange) in the middle of functionally important areas: corticospinal tract (blue), optic tract (yellow) and arcuate fasciculus (green) Bild: Universitätsklinik für Neurochirurgie, Inselspital Bern © CC BY-NC 4.0 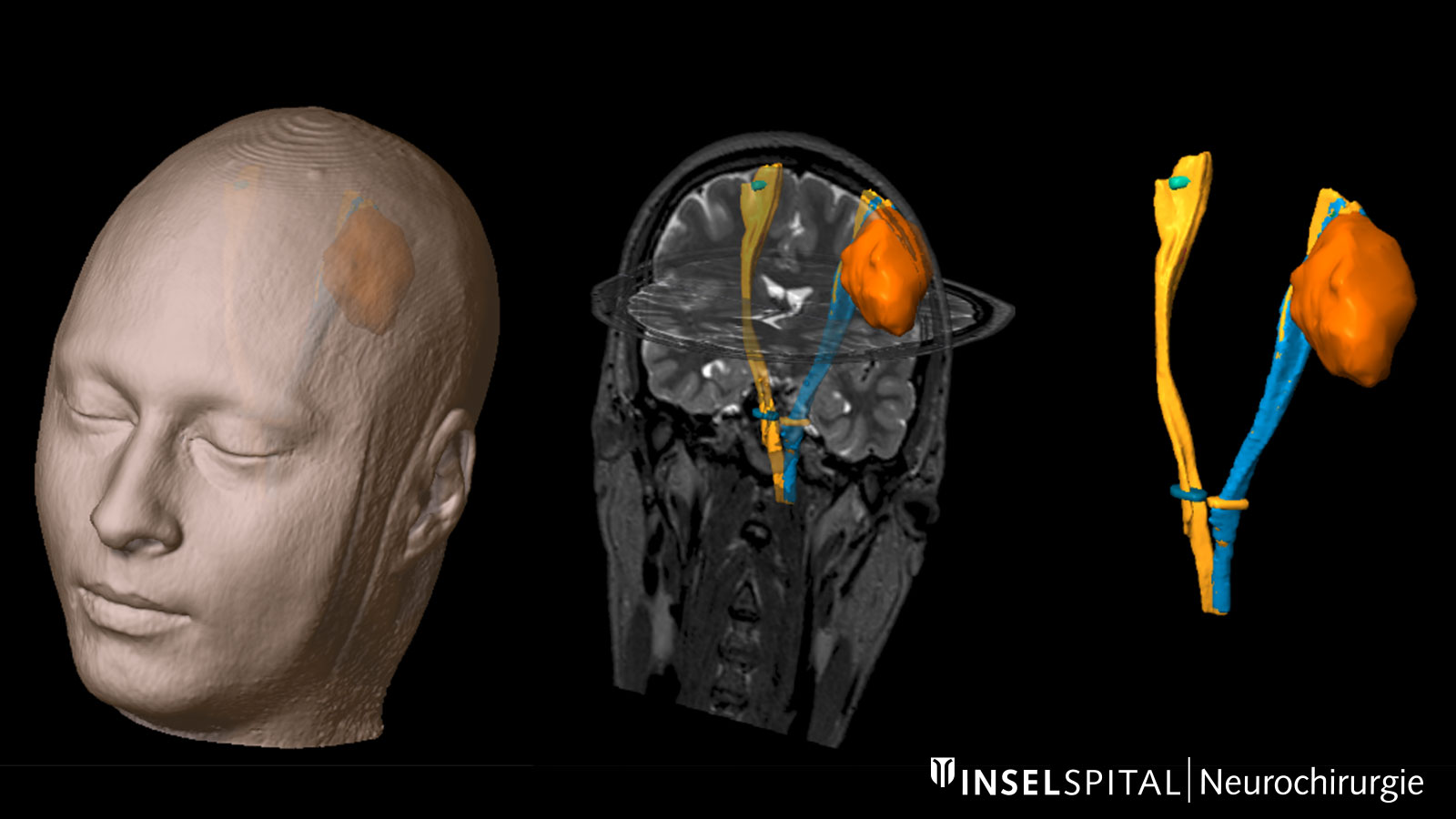
Corticospinal tract. The corticospinal tract (yellow and blue) is shown here as a fiber tract of motor function in relation to a tumor (orange). Bild: Universitätsklinik für Neurochirurgie, Inselspital Bern © CC BY-NC 4.0 
Visual pathway. This illustration shows how the visual pathway (optic tract, green) runs around the ventricular system (purple). Bild: Universitätsklinik für Neurochirurgie, Inselspital Bern © CC BY-NC 4.0 - Fiber tracking for deep brain stimulation
Essential tremor
In essential tremor, we use fiber tracking to visualize the dentatorubrothalamic tract (DRTT) to plan stimulation of functional pathways. This complements traditional purely anatomical planning. The DRTT is located in the posterior subthalamic area (PSA) and is one of the target points in deep brain stimulation (DBS) for the treatment of essential tremor *. Accurate localization is essential in surgical planning to allow precise stimulation of the tract. Fiber tracking can be used to visualize the tract and optimally determine the target points for DBS electrode implantation.

Deep brain stimulation for tremor disease. The left image shows the visualization of the dentatorubrothalamic tract for planning the correct electrode implantation (red) for deep brain stimulation. The right image shows the exact target localization so that the stimulation can take place directly next to the DRTT. Bild: Universitätsklinik für Neurochirurgie, Inselspital Bern © CC BY-NC 4.0 Depression

Deep brain stimulation for depression. The left image shows a 3D reconstruction of the right (red) and left (green) medial forebrain bundle. On the right image, the target points for electrode placement prior to deep brain stimulation are marked as white dots. Bild: Fenoy et. al. 2016, J Affect Disord Another clinical application for fiber tracking at Inselspital is deep brain stimulation (DBS) therapy for severe cases of depression that do not respond to standard therapy. In medical studies, it has been shown that stimulation of the superolateral part of the medial forebrain bundle has a positive therapeutic effect in refractory depression *. In order to correctly identify the fiber bundle and determine the target coordinates for DBS, fiber tracking is necessary prior to the procedure.
")

-
Nowacki A, Debove I, Rossi F, Schlaeppi J, Petermann K, Wiest R, Schüpbach M, Pollo C. Targeting the posterior subthalamic area for essential tremor: proposal for MRI-based anatomical landmarks. Journal of Neurosurgery. 2018;1-8.
-
Fenoy AJ, Schulz P, Selvaraj S, Burrows C, Spiker D, Cao B, et. al. Deep brain stimulation of the medial forebrain bundle: Distinctive responses in resistant depression. J Affect Disord. Oktober 2016;203:143–51.