Tumors of the spinal cord grow slowly and often show few, insidiously developing symptoms until their increasing size causes severe paralysis and gait disturbances. They may grow infiltratively like astrocytoma or have a relatively clear and defined surface like ependymoma. Surgery is the treatment of choice. However, it places the highest technical demands on the neurosurgical team. Spinal cord tumors require specialized surgical and multistage simultaneous monitoring techniques. A new kind of mapping, in the development of which Inselspital was involved, can accurately determine the localization of the trajectory and thereby increase the safety of the procedure.
Which tumors occur in the spinal cord?
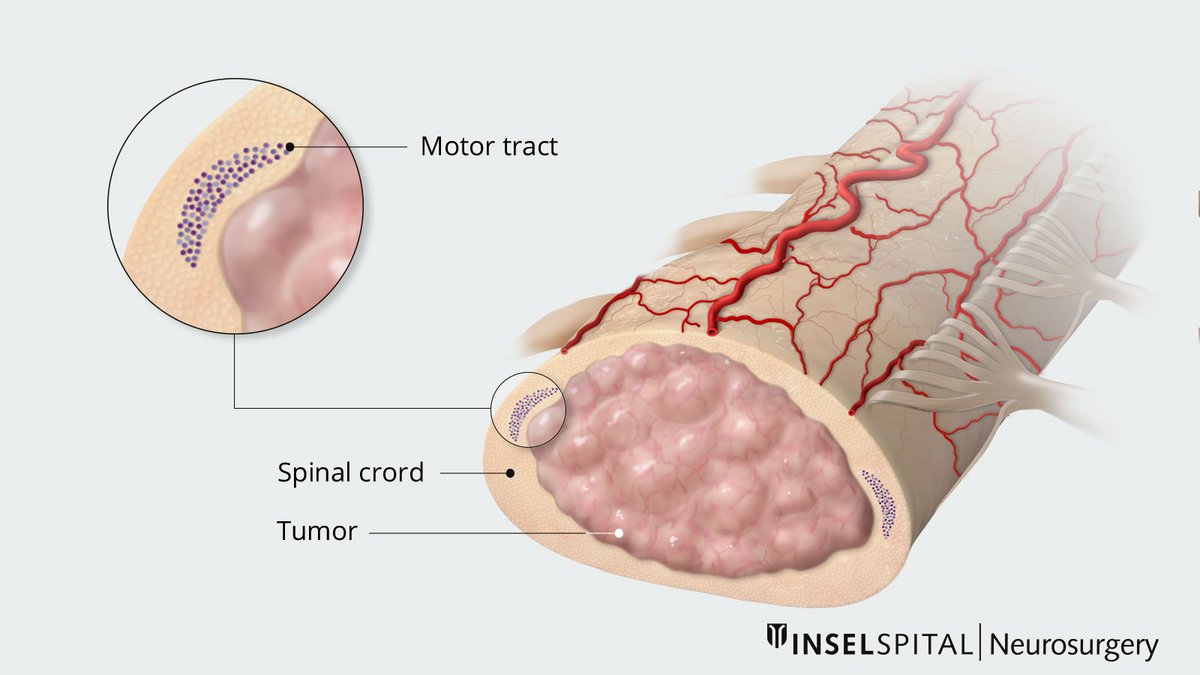
The typical spinal cord tumors are intramedullary ependymomas, astrocytomas, hemangioblastomas, or cavernomas. Intramedullary tumors are located within the spinal cord.
The most common are ependymomas, hemangioblastomas, and cavernomas with mostly smooth surfaces. They can usually – but not always – be completely removed.
Astrocytomas usually have an infiltrative growth pattern, that is, with extensions between the spinal cord tracts. Therefore, they often cannot be removed completely.
What are the risks of spinal cord tumors?
Tumors in the spinal cord grow very slowly and are often benign. However, they are located in one of the most functionally densely packed sites of the nervous system. Without treatment even benign tumors can lead to paraplegia because of the compression of the spinal cord.
In addition, spinal cord surgery is always associated with a serious risk of sensory or motor dysfunction. It is therefore necessary to evaluate the tumor carefully and find the right time for the intervention.
Main risk: paraplegia
Partial, or in the worst case, total paralysis: damage to the spinal cord resulting in paraplegia is the most serious complication following surgery on the spinal cord. Despite careful surgery, it can develop due to a circulatory disruption or mechanical stress. The risk increases with increasing size of the tumor.
Electrophysiological monitoring during the operation is therefore a must.
How is a spinal cord tumor treated?
In the absence of symptoms and for small tumors, except for justified exceptions, a wait-and-see attitude with regular MRI follow-up is appropriate. Intramedullary tumors often grow very slowly, with long pauses, and are sometimes stable for decades.
However, if there are clear symptoms such as numbness, pain, or paralysis, surgery should be performed early because surgical outcomes are better in the early stages and with smaller tumors than with large tumors and already advanced paralysis.
Wherever possible and safe, we perform the operation through a hemilaminectomy approach. For larger exposures, we prefer the technique of laminoplasty with reinsertion of the bony vertebral arches. Both techniques preserve the spinous processes and ligaments, the so-called posterior traction ligament, which is important for the posture and stability of the spine.
Breakthrough in surgical safety
An international research team, including neurosurgeons from Inselspital, has developed a new method for precisely locating key nerve pathways in the spinal cord. The procedure has received scientific recognition and is now routinely used at Inselspital to assist in spinal cord surgeries.
For the safe removal of tumors in the spinal cord, the exact location of the main motor pathway (pyramidal tract) is crucial. It controls voluntary movements and must be spared as much as possible during surgery.
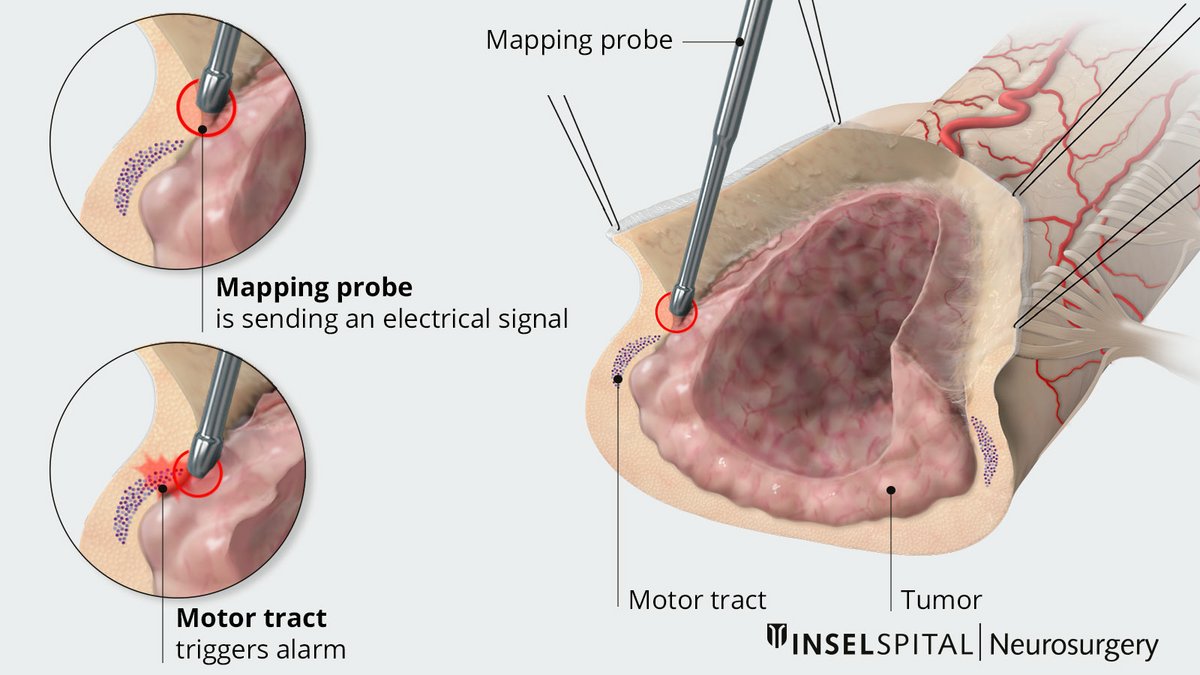
With the new technique known as «Double-Trains» mapping, motor and sensory nerve pathways can now be reliably distinguished for the first time. This is based on their differing response patterns to electrical stimuli in the millisecond range.
This precise localization is particularly important in cases of intramedullary astrocytomas, which grow within the spinal cord and often lack a clear boundary with healthy tissue.
During surgery, the mapping shows how close the surgical site is to important nerve pathways. This allows the procedure to be precisely guided and reduces the risk of neurological deficits. In selected cases involving smaller tumors, complete removal while ensuring safety may also be possible.
What surveillance techniques are used?
Intramedullary tumors place the highest demands on surgery, especially the monitoring of spinal cord function during tumor removal. The ultimate goal of microsurgery is preservation of function with simultaneous complete removal (ependymoma, cavernoma, hemangioblastoma) or maximal reduction (astrocytoma). In addition to specialized instruments and optimized resection technique, neurophysiological monitoring is crucial. Classic neuro-monitoring is not sufficient because the motor evoked potentials are interpreted differently spinally and the sensory potentials are not meaningful for motor function.
Monitoring and mapping
Since the functional density of nerve cells and pathways is greatest in the spinal cord and brainstem, each patient must be fully informed about the possibility of additional neurological disorders. In addition to surgical experience and technique, special intraoperative spinal cord monitoring and now also mapping, which should be performed by a specialized team, help.
Motor-evoked potentials (MEPs)
The electrical stimulation of the motor center sends out impulses that propagate to the muscle via the motor pathway – the tractus corticospinalis – and are transmitted at a velocity of 60 m/s. In the muscle, the responses are derived as curves (motor-evoked potentials) and interpreted by trained personnel. They provide direct feedback on motor functions during the operation.
Somatosensory-evoked potentials (SEPs)
The activity in the dorsal column which carries the signals for sensation and the sense of orientation is measured by somatosensory-evoked potentials (SEP) during surgery. Both pathways must be spared so that the patient does not have any impairments in walking postoperatively.
Vegetative monitoring: In addition, the bulbus cavernosus reflex (BCR) is used to monitor rectal and sexual functions and now also intraoperative bladder pressure monitoring.
D-wave
The D-wave (from direct wave) is the signal directly measured at the motor pathway. Today, it is considered the "gold standard" and decisively determines the strategy of surgery and also the time of a possible termination of the procedure. As long as the D-wave is stably derivable, the patient will not have severe paralysis after surgery or will certainly recover in the course of the next few weeks. This signal has therefore a significant predictive power and has a direct influence on the technique and strategy of surgery.
Follow-up care and prognosis
Surgery is always part of an interdisciplinary treatment plan. Regular follow-up appointments, particularly MRI scans, are important for monitoring the patient’s progress.
Depending on the tissue diagnosis, radiation therapy or chemotherapy may follow surgery for malignant tumors or be used to supplement treatment for inoperable tumors. In many cases, however, surgery alone is sufficient.
Even if a small residual tumor remains after surgery, it often grows very slowly or remains stable for many years.
Rehabilitation
A central component of treatment is specialized neuro-rehabilitation, either on an outpatient or inpatient basis, for example at our Riggisberg Hospital.
Early and consistent rehabilitation can significantly improve existing neurological deficits and support functional recovery.
Further reading
- Deletis V, Seidel K, Sala F, Raabe A, Chudy D, Beck J et al. Intraoperative identification of the corticospinal tract and dorsal column of the spinal cord by electrical stimulation. Journal of Neurology, Neurosurgery & Psychiatry. 2018;89(7):754-761.
- Deletis V, Seidel K. Intraoperative Neurophysiology during Surgery for Spinal Cord Tumors. Spinal Cord Tumors. Springer; 2019. p. 109-125.
- Deletis V, Shils JL, Sala F, Seidel K. Neurophysiology in Neurosurgery: A Modern Approach. 2020