Sufficient and continuous blood flow is essential for our brain. It needs about 20% of the total stroke volume of the heart for its normal function. If a vascular disease leads to reduced blood flow in the brain a stroke can occur. Common causes of cerebrovascular disease are narrowing of the arteries supplying the brain due to arteriosclerotic deposits. If certain diagnostic criteria are met, surgical treatment is possible.
How does the blood supply to the brain work?
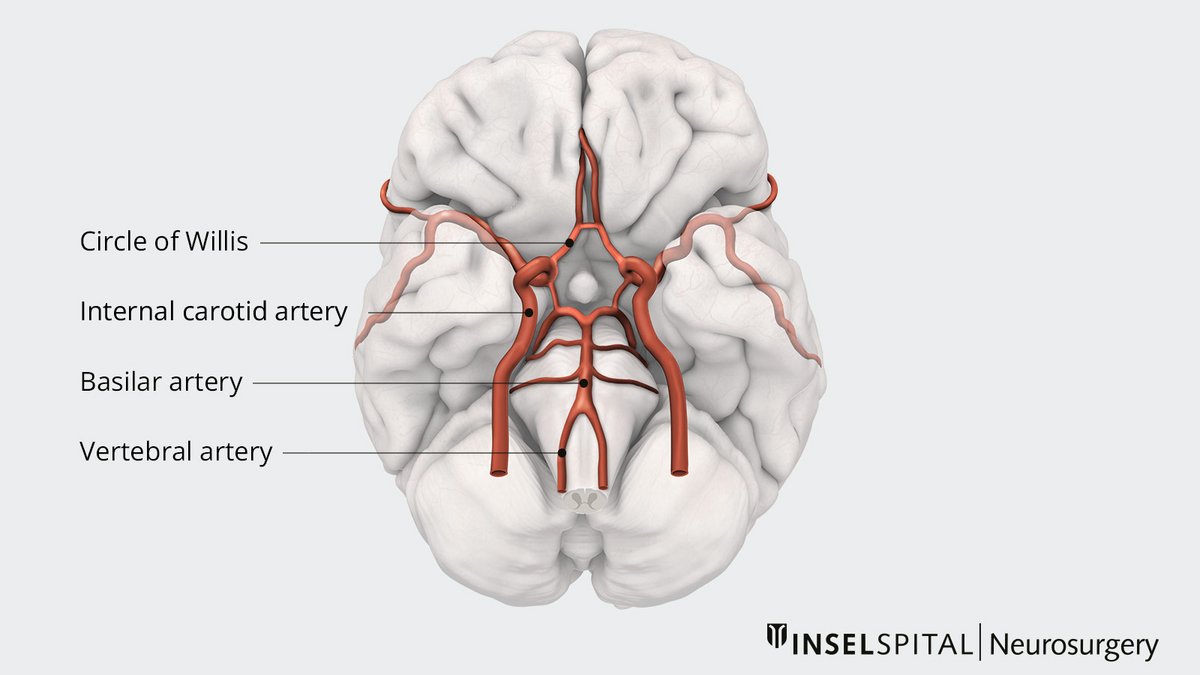
The brain is supplied with blood by two pairs of arteries (left and right): the internal carotid artery (arteria carotis interna) which supplies the anterior circulation of the brain and the vertebral artery (arteria vertebralis) for the posterior supply. After entering the skull bone, the right and left vertebral arteries join to form a single artery, the basilar artery. At the base of the brain, these vessels form a vascular circle, the circle of Willis, via cross-connections. Despite this circle, each of these vessels supplies blood to a specific part of the brain.
What is cerebrovascular disease?
Cerebrovascular disease occurs when the brain can no longer be supplied with sufficient blood. The causes for this are manifold. Restrictions in blood flow may occur from vessel narrowing (stenosis), clot formation (thrombosis), blockage (embolism) or blood vessel rupture (hemorrhage).
Typical risk factors for atherosclerotic deposits which cause stenosis include smoking, high blood pressure, elevated blood lipid levels and diabetes mellitus. More rare causes are diseases such as Moyamoya disease.
The therapy often consists of optimal treatment of the risk factors or endovascular therapy. However, carotid stenosis in particular, but also other circulatory disorders, can also be treated surgically.
In the case of circulatory disorders that originate inside the skull and cannot be treated by endovascular therapy, a cerebral bypass must be considered. For successful therapy, it is indispensable to classify patients according to the severity of their disorder.
How is cerebrovascular disease classified?
A distinction is made between 3 stages of hemodynamic restriction:
Stage I
During the first stage, the body counteracts the reduced blood flow to the brain by dilating the vessels and thus increasing the transported blood volume. Cerebral autoregulation - blood flow control in the brain - is utilized to the maximum.
Stage II
In the second stage, the widening of the vessels is no longer sufficient to counteract the reduced blood flow. More oxygen is extracted from the blood. In medical terms, this is referred to as increased oxygen extraction. However, the cerebral metabolism can still be maintained.
Stage III
In the last stage, both the widening of the vessels and the increase in oxygen extraction from the blood are no longer sufficient. Cerebral metabolism can no longer be maintained. The result is a stroke.
How is cerebrovascular disease diagnosed?
Depending on the localization of the reduced blood flow, the patient's symptoms and the phase of the restriction, various examinations can be considered. The type of examination depends largely on the problem. For example, xenon CT, transcranial Doppler (TCD), single photon emission computed tomography (SPECT) or magnetic resonance imaging (MRI) can be used to determine cerebral autoregulation (stage I). The rate of extracted oxygen can be determined by positron emission tomography (PET) (stage II).
Positron emission tomography (PET) is a diagnostic imaging technique that can effectively visualize pathological changes. At the end of 2020, the world's fastest PET-CT scanner was put into operation at the University Department of Nuclear Medicine at Inselspital. This scanner of the very latest technology enables excellent examination quality with shorter examination times and reduced radiation exposure for our patients.
How is a cerebrovascular disorder treated?
An extracranial-intracranial bypass is available as a surgical procedure for intracerebral vascular stenoses. In this case, an extracranial vessel is connected to a vessel in the brain via an opening in the skull (bypass). In this way, a narrowed vessel can be bridged and the blood supply to the brain can be improved.
In principle, a distinction must be made between bypasses that support the blood supply in a specific area of the brain and bypasses that take over the blood supply completely. In the case of bypasses that are intended to support the blood supply, a lower blood flow is sufficient. In these cases, one speaks of a standard-flow bypass. If larger blood flows have to be achieved or the entire blood supply has to be replaced, an intermediate-flow or high-flow bypass has to be performed.
Type I standard flow bypass
For a standard flow bypass, an artery in the scalp, e.g. the superficial temporal artery, is surgically connected to a cerebral artery, usually the middle cerebral artery. The amount of blood transported via this bypass can be 20–70 ml/min. The 5-year open rate of this bypass is about 95%.
Type II intermediate flow bypass
For an intermediate-flow bypass, an artery of the arm, usually the radial artery, is excised and connected to the external carotid artery at the neck. The vessel is then tunneled under the skin to the head and connected to a larger, slightly lower branch, such as the middle cerebral artery. About 60–100 ml/min can be transported via an intermediate-flow bypass. The 5-year open rate for this bypass is about 90–95 %.
Type III high flow bypass
In a high-flow bypass, a large-caliber leg vein such as the saphenous vein is excised and connected to the internal carotid artery or also the common carotid artery in a similar way to the intermediate-flow bypass at the neck and then led to the skull. Here, a connection is usually made in the depth of the brain with the main branch of the arteria cerebri media. About 100–200 ml/min can be transported via a high-flow bypass. The 5-year open rate is approx. 80–85%.