Spinal stenosis of the lumbar spine is a common cause of difficulty walking in older adults and is often overlooked. The narrowing of the spinal canal leads to compression of the nerves, causing pain, weakness, or sensory disturbances in one or both legs, usually after walking for just a few minutes. Studies show that microsurgical removal of the excess tissue relieves pressure on the nerves, produces immediate results, involves few complications, and leads to significant, long-term improvement in eight out of ten patients.

How does a narrowing of the spinal canal occur?
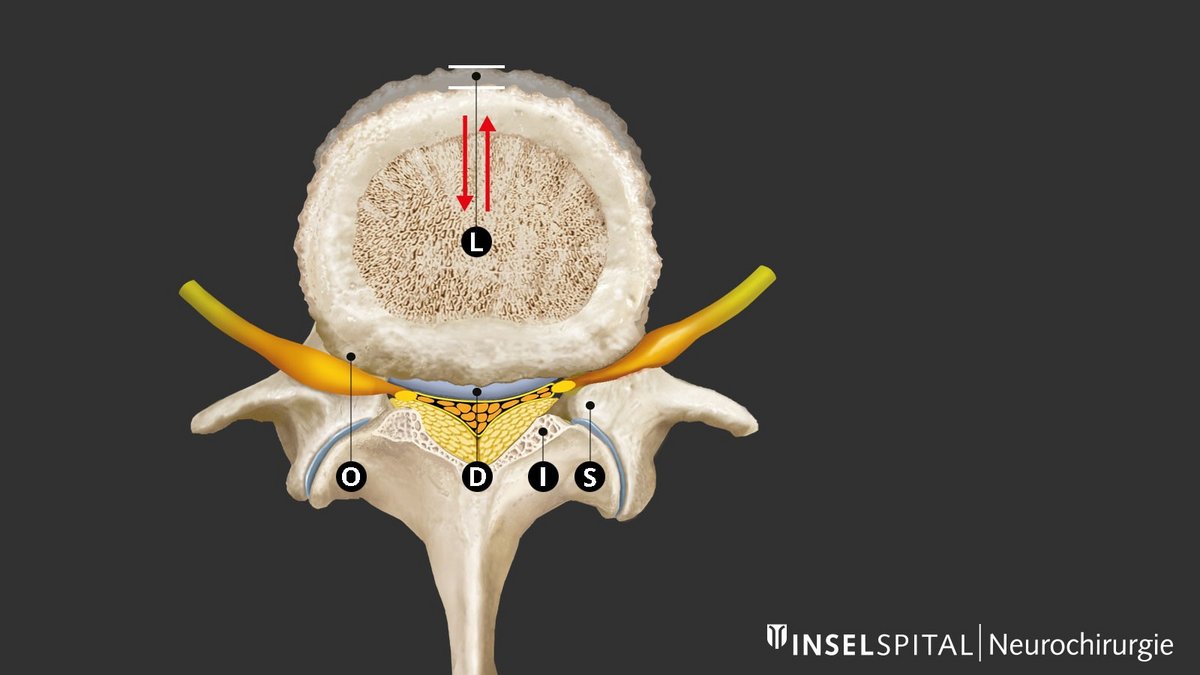
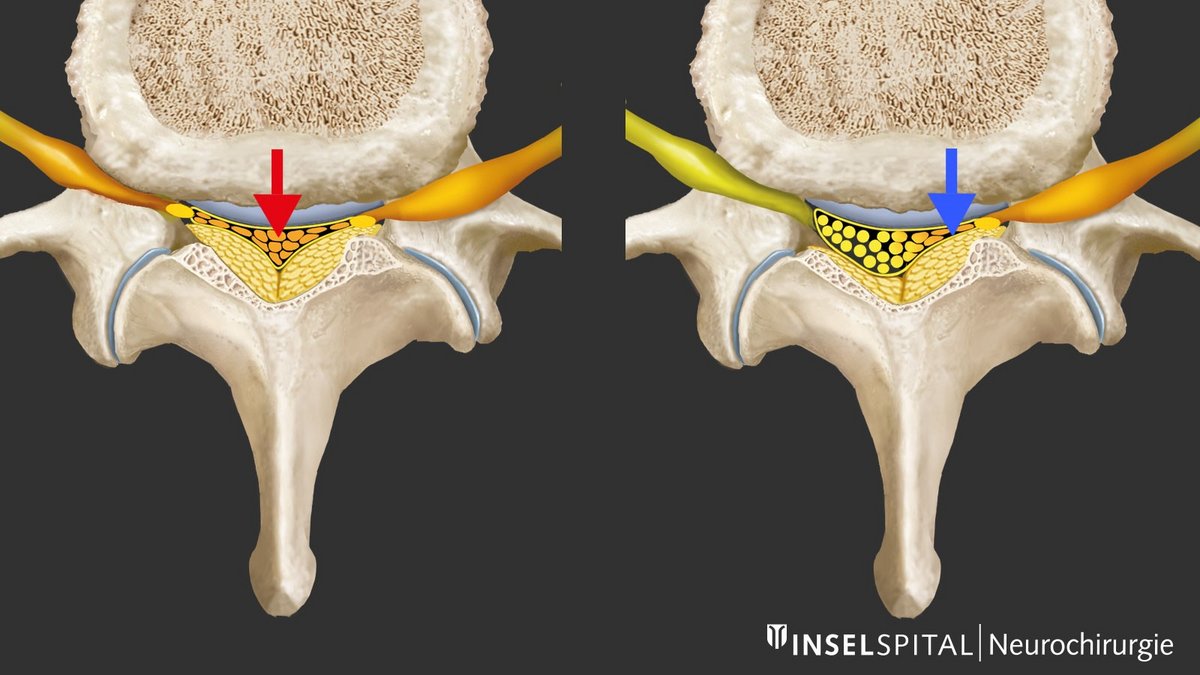
As the spine wears and ages, degenerative changes occur, which are most pronounced in the lower lumbar spine. A key role is played by dehydration of the intervertebral disc with loss of height and micromovements between two vertebra. The body reacts by trying to restabilize the spine through thickening of the ligamentum flavum and bone build-up or hypertrophy, especially at the facet joint. This causes central and lateral narrowing of the spinal canal and the intervertebral foramina with compression of the nerves centrally, recessively (recess stenosis) and less often foraminally when exiting the foramen. This stenosis of the spinal canal can be exacerbated by bulging of the intervertebral disc or, in rare cases, by vertebral slippage.
How common is spinal stenosis?
There are no reliable figures on the frequency of spinal stenosis. Except where constriction of the spinal canal is congenital, the disease typically occurs in the elderly. Women are more often affected than men (ratio 3:1). A radiologically narrow spinal canal occurs in 20–40% of older people. About 1–5% of all older patients with back pain have spinal stenosis that requires treatment. Stenosis can also arise within a relatively short time. Therefore, it may be advisable to have a repeat MRI after 2–3 years.
After operations on herniated discs, microsurgical treatment for spinal stenosis is the second most common back operation (13 operations per 100,000 inhabitants per year) and the most common operation for patients over 50 years of age.
Factors like the increasing life expectancy, the higher proportion of older people in the general population and the desire to continue an active lifestyle into old age are reasons why the clinical picture of spinal stenosis will gain in importance in the coming years.
What are the symptoms of spinal stenosis?
Typical complaints and key symptoms include:
- Difficulties with walking accompanied by weakness or pain in the buttocks and/or leg, on one or both sides
- Back pain (lumbago) of varying intensity
- Improvement in symptoms when bending forward or sitting down
Claudicatio spinalis
Classic lumbar spinal stenosis manifests as pain in one or both legs that occurs after walking a certain distance or standing for a prolonged period. Medical professionals refer to this as neurogenic claudication or spinal claudication. The leg pain may be accompanied by back pain.
A characteristic feature is that the pain improves when sitting, lying down, or cycling, but not simply by standing still. This is how spinal claudication differs from intermittent claudication. Leaning forward, for example while leaning on a shopping cart, also often provides significant relief.
Some patients experience leg pain in any body position when their back is straight, as extension of the spine reduces the internal diameter of the spinal canal, while flexion increases it. Therefore, cycling is generally well tolerated.
However, typical spinal claudication does not occur in 30% of patients. Instead, sciatica-like pain, sensory disturbances such as tingling, calf cramps, weakness in the legs, or pain at rest may be the primary symptoms.
Back pain
Back pain is a common symptom, but its severity varies and is often related to physical activity. In rare cases where spondylolisthesis is present, the pain may be the primary symptom due to spinal instability. Back pain is also often caused secondarily by maintaining a protective posture that involves leaning forward.
Neurological deficits
Sensory, motor, and reflex disturbances—if they occur at all—tend to be mild. The areas supplied by the L5 nerve root (e.g., weakness in the foot flexors or reduced sensation in the big toe region) or the L4 nerve root (e.g., weakness of the thigh extensor/quadriceps or reduced sensation on the inner side of the lower leg). Other nerve roots are affected less frequently.
In many cases, the neurological examination is unremarkable. Acute paralysis can occur, but is rare.
So-called cauda equina syndrome, with bladder or rectal dysfunction due to compression of the dural sac, is very rare.
How is spinal stenosis diagnosed?
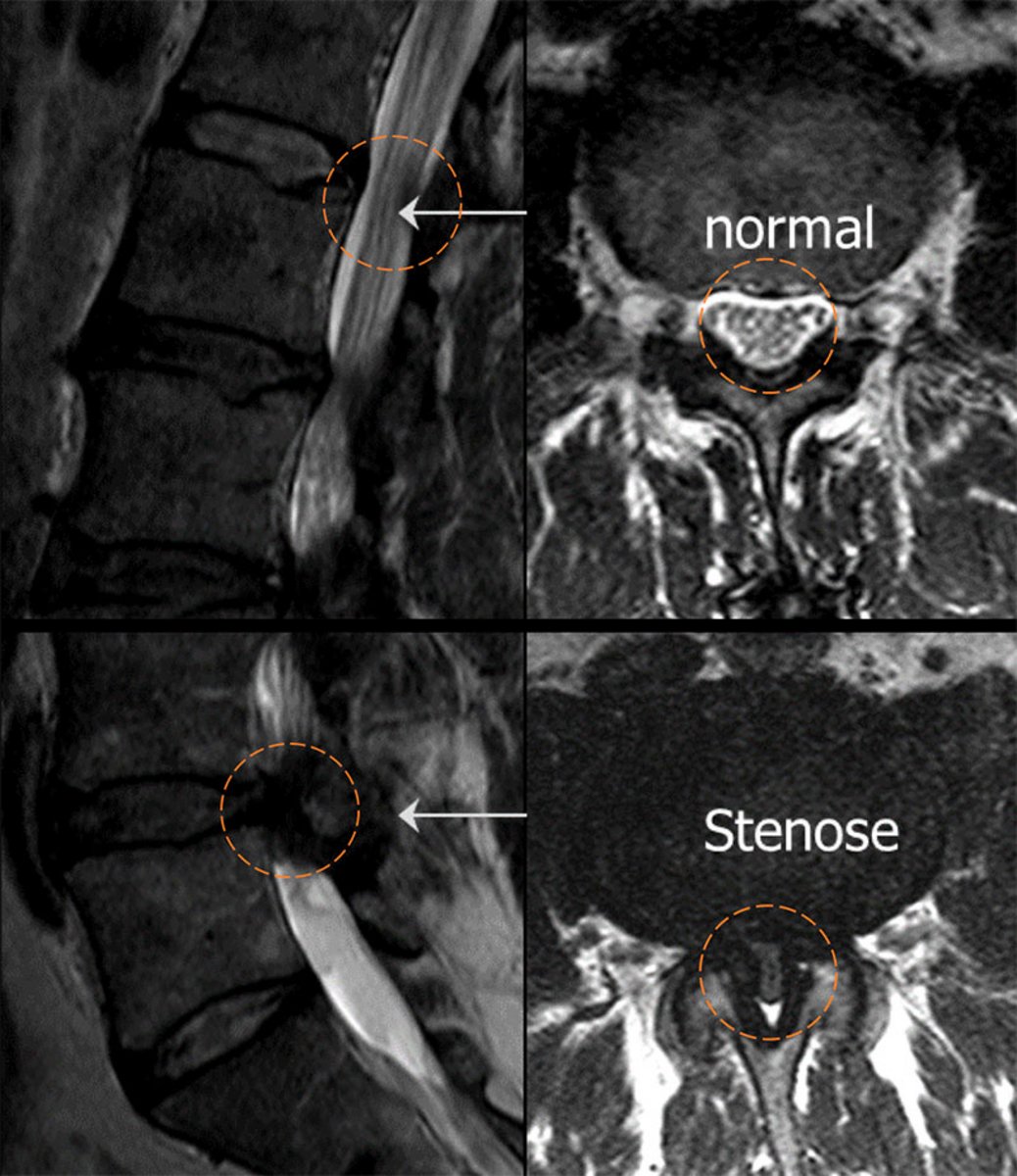
Magnetic resonance imaging (MRI) of the lumbar spine is the examination of choice. MRI often reveals thickening of the spinal ligaments (ligamenta flava) as well as enlarged intervertebral joints, which lead to a significant narrowing of the spinal canal. A mild to moderate protrusion of the intervertebral disc is also frequently visible. The L4/L5 or L3/L4 segments are usually affected.
In cases of a congenitally narrow spinal canal, multiple narrowings are already present by middle age.
If back pain is the primary complaint, a functional assessment of the lumbar spine in flexion and extension may be useful to confirm or rule out spondylolisthesis.
Vascular intermittent claudication should be ruled out based on typical clinical signs or via Doppler examination. Typical indications include absent foot pulses, trophic skin changes, cold skin, symptoms even in a flexed position (e.g., while cycling), and pain that is more muscular than nerve-related.
Getting a second opinion

The decision on whether to have an operation on your spine is not always easy. There are often several possible surgical methods to choose from, each with different advantages and risks that need to be weighed up. A second opinion helps you to make the right decision for you and confirms that your treatment reflects the state-of-the-art in medicine. Make an appointment with us at the neurosurgical polyclinic or arrange a consultation with the chief physician.
How is spinal stenosis treated?
Around 20–40% of people over the age of 60 years show signs of spinal stenosis on X-rays but report no complaints. In these cases, treatment is not necessary.
However, for people with obvious symptoms, surgery should be considered. In particular, for older patients with clear symptoms, the operation should not be postponed for too long; otherwise they will suffer loss of stamina due to increasing immobility and will become weaker.
The operation is a routine procedure with a low complication rate – even for 70- to 90-year-old patients. Therefore, surgery is the treatment of choice even in elderly people.
Minimally invasive surgery for spinal stenosis
During surgery for spinal stenosis, the narrowing is removed under a surgical microscope, the compressed nerves are released, and the internal diameter of the spinal canal is restored.
Over time, the surgical technique used has increasingly evolved toward minimally invasive procedures. At Inselspital, a combination of a small access route (“keyhole technique”), muscle- and joint-sparing techniques, and preservation of mobility is now used. Spinal fusion is generally not necessary.
The spinous processes and the posterior ligamentous structures of the spine are preserved as much as possible. This results in only a small incision, and the stability of the spine is largely preserved.

Modern minimally invasive microsurgical techniques
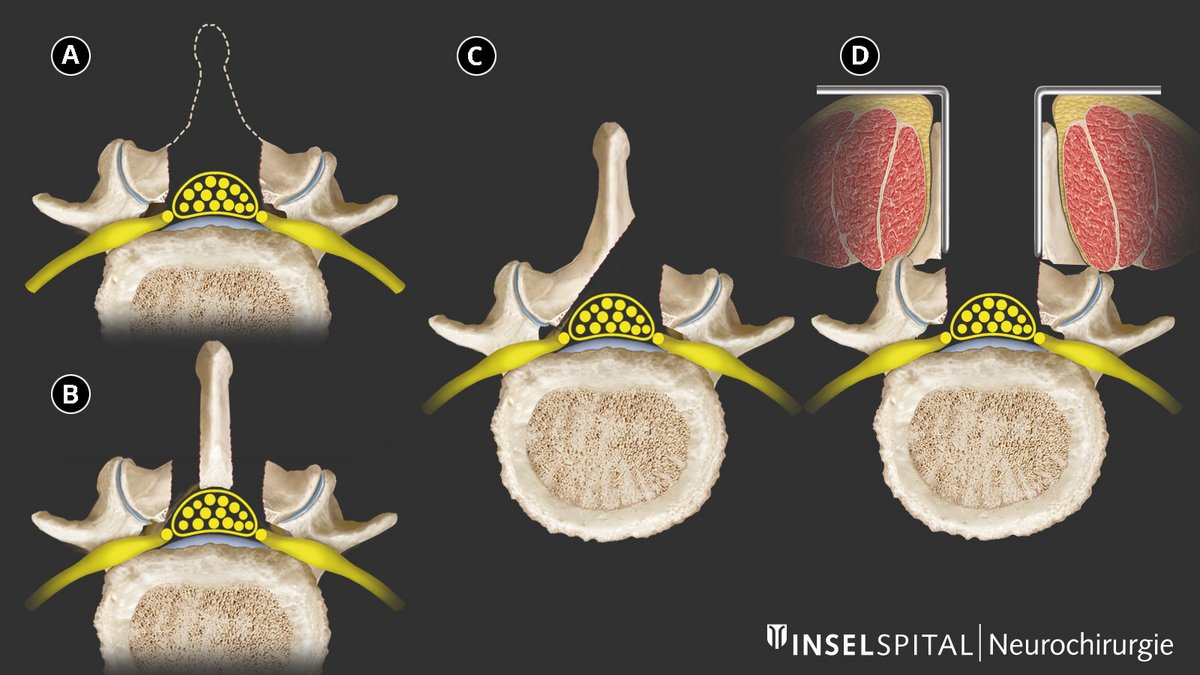
Traditional laminectomy, in which the entire posterior wall of the spinal canal (spinous process and vertebral arch) is removed in the affected segment, is now considered outdated. This procedure can compromise the stability of the spine and is not minimally invasive.
Modern procedures aim to remove only the constricting bone and ligament tissue that is pressing on the nerves. This is done either through an approach via the spinous process or via a unilateral or bilateral approach. In this process, the spinous process, stabilizing ligaments, and vertebral arches are preserved as much as possible.
The choice of access technique depends on the MRI imaging as well as the patient’s overall condition.
An additional access route via a tubular system (tubular technique) allows for further preservation of the musculature and makes the procedure even less invasive.
Do vertebrae have to be screwed and fused?
Spinal fusion and spinal fusion surgery are generally not necessary for spinal stenosis. In most cases, the condition involves a simple narrowing of the spinal canal without significant spinal instability.
In some cases, however, spinal fusion is considered out of concern that the surgery itself might cause instability. This applies, however, to only a small minority of patients. Studies have shown that after minimally invasive decompression, only about 3% of patients subsequently required additional surgical fusion due to instability *.
Even in cases of mild vertebral displacement (up to about 3 mm on dynamic imaging), primary fusion can often be avoided *.
Another argument against fusion is that the adjacent vertebral segments are subjected to greater stress and may wear out more quickly over time (in about 3–4% of patients who undergo fusion surgery). This can lead to further symptoms and repeat surgeries over time. This rate is higher than the incidence of instability following a previous minimally invasive decompression surgery.
What is the success rate of this surgery?
Most patients, about 7–8 out of 10 (70–80%) feel the beneficial effects of the surgery straight away. The pain is noticeably reduced, and the distance the patient can walk normalizes or is significantly extended. This improvement usually lasts for years. The success of the operation is most evident in the reduction of leg pain, but back pain also often disappears.
It is important to remember that the spine remains the same and occasional residual complaints are unavoidable. In addition, new degenerative changes can arise over time. It is assumed that about 10% of the patients will have to be operated on again after about 5 years, mostly due to further wear on the neighboring vertebrae or on the operated segment itself.
In 2 out of 10 patients, significant residual symptoms remain or recur. The causes are nerve-related pain, residual pain emanating from the spine or the formation of scar tissue.
What are the surgical risks?
Microsurgical decompression is very safe even in elderly patients. Severe and persistent complications affect only 1 in 100 patients (1%). This includes injuries to the nerves, heart attacks, pulmonary embolism and other rare life-threatening incidents. This extremely low number of complications has been confirmed in several international studies.
Mild and temporary complications that do not cause any permanent damage include:
- Leakage of cerebrospinal fluid from the dural sac in 1 in 20 patients (5%). This is due to adhesion of the dural sac to the stenosis. This usually very small leak is sealed immediately during the operation.
- Bleeding in 1 in 50 patients (2%). In some cases, the bleeding needs to be stopped by a simple second operation.
- Infection in 1 in 50 patients (2%). If infection develops, antibiotics are given and the wound is cleaned.
The mortality rate within 90 days after the operation – a marker of the severity of the procedure – is only 2 in 1,000 patients (0.2%) despite the older patient age of 60–90 years *.
What happens after the surgery and how long is the hospital stay?
The surgery is performed under general anesthesia and takes about 30 to 60 minutes per segment. Patients are then monitored in the recovery room for approximately 4 hours before being transferred back to the ward.
With the assistance of a nurse, patients are usually able to get out of bed for the first time on the same day. The day after surgery, patients receive guidance from physical therapy, with mobilization beginning as soon as possible.
Local wound pain may still occur. However, in about 8 out of 10 patients, leg pain is significantly improved or gone immediately after the surgery, so that walking independently and climbing stairs is usually possible again quickly.
If necessary, pain relievers such as acetaminophen, Novalgin, or ibuprofen are used.
The hospital stay is usually 2 to 5 days, depending on symptoms, support at home, and the individual’s recovery. Subsequent inpatient rehabilitation is normally not required.

What happens after discharge from the hospital?
We recommend gradually returning to normal mobility within the first few days after surgery. However, the return to daily activities and physical exertion depends heavily on your age, overall health, any underlying medical conditions, and residual symptoms.
Even if longer walks are possible after discharge, strenuous physical activity, heavy lifting, and movements involving twisting or significant bending of the spine should be avoided during the first 4–8 weeks to ensure proper internal wound healing.
Light swimming and careful jogging are generally possible starting about 3 weeks after surgery.
Physical therapists provide information on posture, movement, and back exercises during your hospital stay and provide relevant informational materials. Outpatient physical therapy may be beneficial afterward but is not mandatory. Inpatient rehabilitation is only necessary in exceptional cases.
For patients who live alone and require assistance, we can also arrange for a home care aide if needed.
Non-surgical treatment
Conservative treatment is only partially effective, as the symptoms are caused by compression of the nerve roots. Measures such as back training, physical therapy, an adapted activity plan, and pain relievers (e.g., acetaminophen, anti-inflammatory drugs, flupirtine, or gabapentin) can temporarily relieve symptoms.
Injections of local anesthetics and corticosteroids (e.g., triamcinolone) into trigger points or facet joints can also provide short-term relief. In many cases, however, the effect wears off after some time.
As a rule, in cases of persistent and severe symptoms, surgical decompression of the compressed nerves is necessary to achieve long-term improvement. This has been scientifically proven in several studies.
Study comparing surgery with conservative treatment
Surgery yields better results than conservative treatment for patients with spinal stenosis. The results of the biggest prospective randomized controlled study comparing surgery with conservative management shows this clearly *. This investigation provides the strongest medical evidence for the benefits of spinal stenosis surgery. The benefits of the operation also continue for many years *.
Are there alternative surgical procedures?
Interspinous spacer
Another minimally invasive procedure consists of the implantation of an interspinous spacer. The spacer is implanted between two interspinous processes. This implant forces the affected segment into an (unnatural) forward bend, a so-called kyphosis. In this way, the internal diameter of the spinal canal is increased. However, this process is characterized by a high failure rate over the long term and should only be performed as an exception in patients with a high general surgical risk. In the medium term, it also leads to increased wear and tear of the surface of the vertebral segments.
Instrumentation and fusion
These technical terms refer to the screwing and stiffening of a section of the spine. This includes surgical interventions performed from the front, the side and most often from behind, the latter with the implantation of at least 4 screws in adjacent vertebrae. These screws are connected with titanium rods to bring the vertebrae back into the correct position and stabilize them. For permanent fusion the intervertebral disc would also be removed and replaced with an implant (spacer). This additional support prevents the screws from gradually loosening and breaking.
So-called dynamic stabilizations have also been used, but they ossify over time and have therefore not become established in practice.
The insertion of screws and the removal of the intervertebral disc with fusion is only necessary if, according to defined criteria, overt mobile instability, so-called spondylolisthesis, is visible on the MRI scan and the corresponding symptoms are present. However, this condition does not affect more than 5% of patients. If in doubt, patients should seek a second medical opinion.
-
Schär RT, Kiebach S, Raabe A, Ulrich CT. Reoperation Rate After Microsurgical Uni- or Bilateral Laminotomy for Lumbar Spinal Stenosis With and Without Low-grade Spondylolisthesis. SPINE. 2019;44(4):E245-E251.
-
Peul W, Moojen W. Fusion for Lumbar Spinal Stenosis – Safeguard or Superfluous Surgical Implant?. New England Journal of Medicine. 2016;374(15):1478-1479.
-
Weinstein J, Tosteson T, Lurie J, Tosteson A, Blood E, Hanscom B et al. Surgical versus Nonsurgical Therapy for Lumbar Spinal Stenosis. New England Journal of Medicine. 2008;358(8):794-810.
-
Weinstein J, Tosteson T, Lurie J, Tosteson A, Blood E, Herkowitz H et al. Surgical Versus Nonoperative Treatment for Lumbar Spinal Stenosis Four-Year Results of the Spine Patient Outcomes Research Trial. Spine. 2010;35(14):1329-1338.
Further reading
- Raabe A, Beck J, Ulrich C. Nötig oder unnötig? Rückenoperationen im kritischen Blick. Therapeutische Umschau. 2014;71(12):701-705.
- Raabe, A, Ulrich, CT, Schär, RT. Immobil durch spinale Stenose : das neue alte Volksleiden. Revue medicale suisse. 2019;15(636):292–294.
- Schär RT, Pollo C, Ulrich CT, Raabe A. Zervikale und lumbale Radikulopathien. Swiss Medical Forum ‒ Schweizerisches Medizin-Forum. 2019;