A cerebrospinal fluid leak or short CSF leak causes headaches in patients when they are in an upright position. Spontaneous recovery is common. However, if symptoms persist unchanged after 3–4 weeks, a special evaluation is needed. If this reveals the exact location of the leak, surgical occlusion should be performed, because otherwise the headache may progress to a chronic stage. Timely diagnosis and therapy are therefore very important.
What is special about a CSF leak?
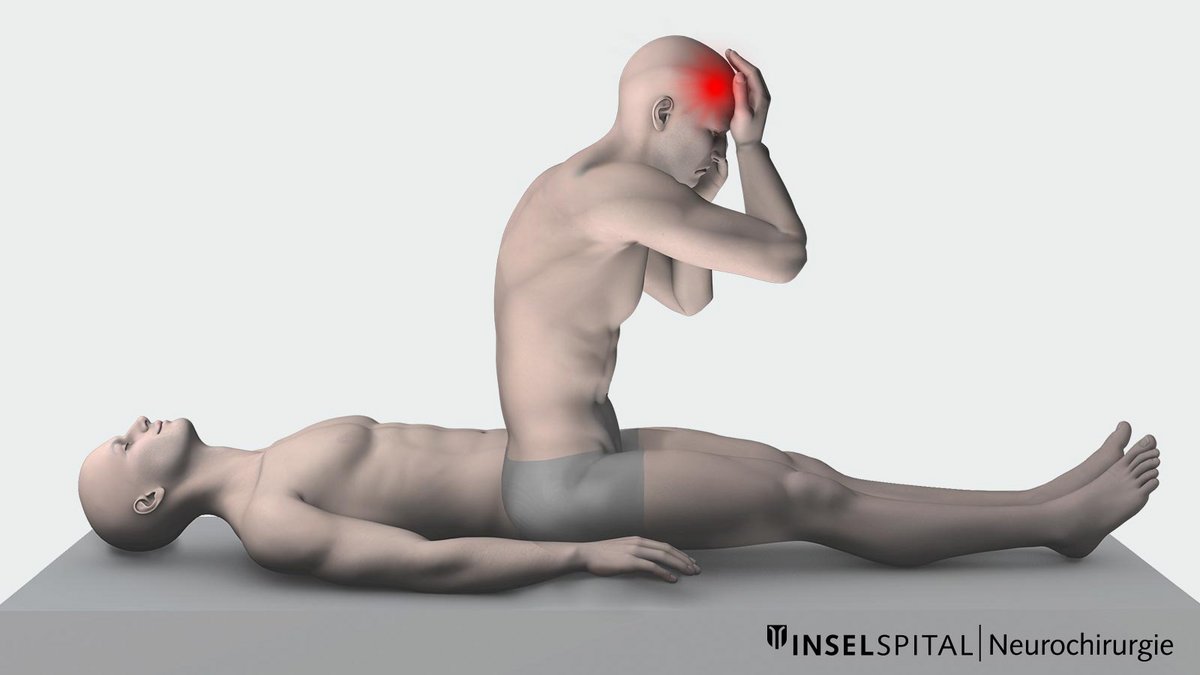
A cerebrospinal fluid leak is not a new, but an increasingly frequently diagnosed condition. The most important symptom is orthostatic headache - that is, a headache that begins immediately after changing position to a more upright position (from lying to standing or from lying to sitting) and improves rapidly after lying down. Most often, CSF is lost through an unnoticed defect in the meninges of the spinal cord, the spinal dura.
Synonyms
There are numerous English and German names and abbreviations for the disease. The official name is spontaneous intracranial hypotension (SIH). Other names are listed here:
| Cerebrospinal fluid hypotension syndrome | Low-ICP syndrome | Spinal headache |
| Hypoliquorrhea syndrome | CSFL | Orthostatic headache syndrome |
| Spinal cerebrospinal fluid leak syndrome | Low pressure headache | Spontaneous spinal CSF fistula |
What is the cause of cerebrospinal fluid leak syndrome?
The cause is usually a cerebrospinal fluid leak in the spine. The most noticeable symptom, however, is orthostatic headache—meaning the problem originates in the back but is felt primarily in the head.
The brain and spinal cord "swim" embedded and well protected against vibrations in about 140 ml of cerebrospinal fluid, also called brain or nerve fluid. About 500 ml of this fluid is newly formed and also broken down again every day. The meninges of the brain and spinal cord make this closed system virtually "watertight".
A small tear in the spinal cord skin leads to leakage of CSF into the spinal canal and from there into soft tissues such as muscles and fatty tissue. In very rare cases, there are also vascular connections from which the CSF directly enters the venous system.
Causes for a small tear of the spinal dura and for CSF leak may be:
- violent coughing or sneezing attacks
- minor injuries such as bruises, sprains or abrasions
- strong, abrupt movements
- a sharp bone spur on the spine that bores a hole in the skin of the spinal cord. A bone spur occurs, for example, due to wear and tear when joints or vertebrae rub against each other
The loss of cerebrospinal fluid is most noticeable in the upright position and hardly ever in the supine position. When a patient stands up, cerebrospinal fluid is drained again, and the already small amount of cerebrospinal fluid shifts toward the spine and is then missing from the head. The brain now no longer floats in the water, but rests on the base of the skull and deforms. If the patient lies down again, the water shifts back toward the head. This explains why patients have discomfort in an upright posture, especially when standing, and feel relief from the headache when they lie down again.
What are the symptoms of a CSF leak?
When standing, the brain sags into the bony skull. The spectrum of symptoms caused by this is very wide. It ranges from mild headaches at the end of the day to massive discomfort only seconds after standing up.
The pull on the meninges and vessels causes headaches, sometimes also nausea, dizziness, sensitivity to light and noise. If cranial nerves and pituitary stalk are involved by the pull, this can also cause symptoms: double vision, visual disturbances, cardiac arrhythmias, hearing disturbances, etc. In extreme cases, consciousness is affected.
A hygroma, the accumulation of fluid between the meninges of the skull, can also be a consequence of the sagging of the brain. As a feared complication, bleeding in these spaces, so-called subdural hematomas, can also occur.
This is how patients describe the unusual symptoms
- "A shooting pain from the top of my head down the back of my neck."
- "I felt like I was drunk."
- "I was unable to get out of bed or even lift my head a little. "
- "Everything was ringing, I felt like I was inside a box."
- "A dull feeling like being underwater."
- "I was like a paraplegic."
How is a CSF leak diagnosed?
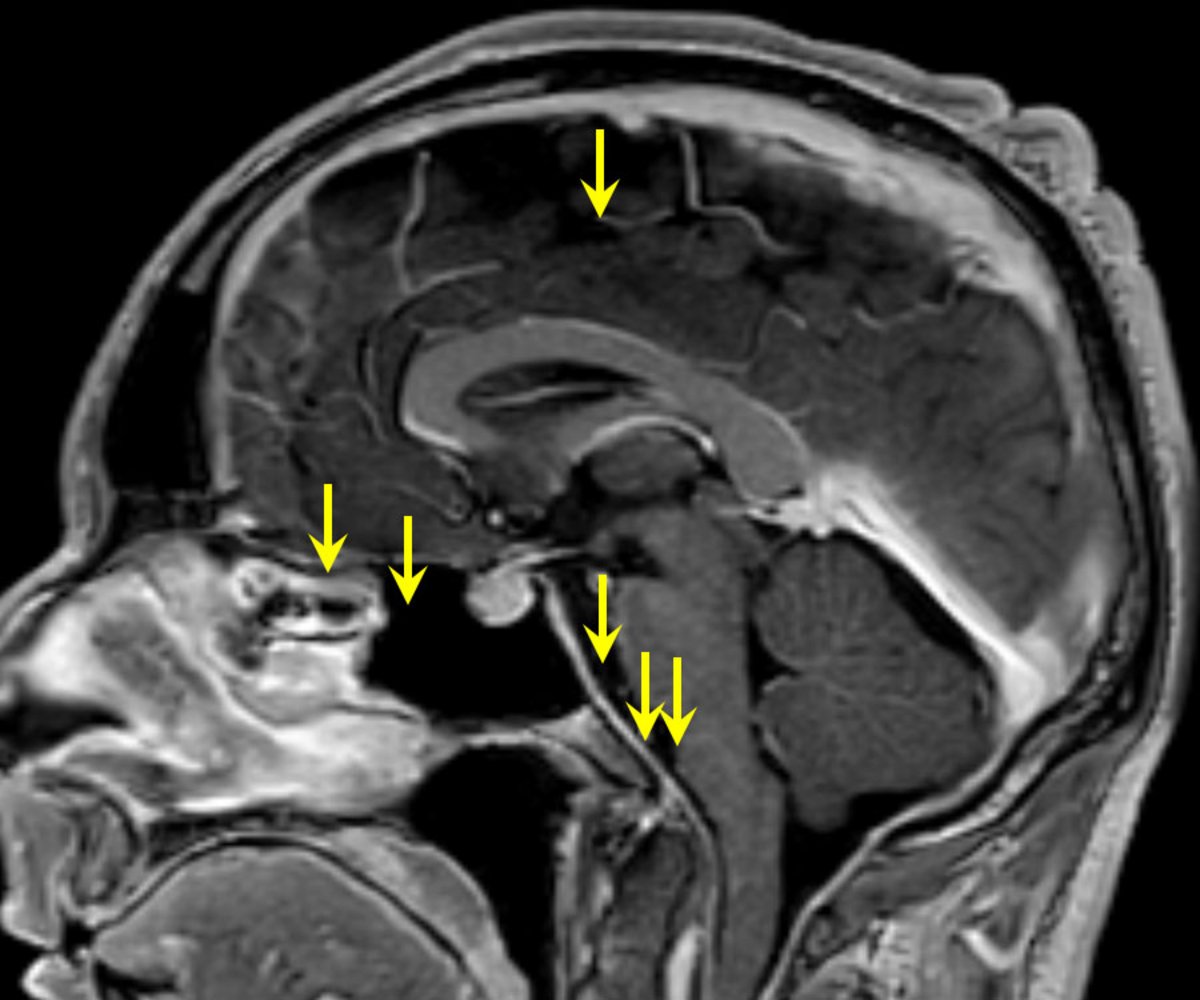
Due to the symptoms, the affected patients usually undergo an imaging procedure such as magnetic resonance imaging (MRI). According to the assessment scheme developed by us (PDF), 6 indirect signs of CSF hypotension syndrome can be observed:
- Contrast enhancement of the dura
- Subdural fluid accumulation (subdural hematomas and hygromas)
- Congestion (buildup) of the large venous structures
- Hyperemia of the pituitary gland leads to reduction of the suprasellar cistern (< 4 mm).
- Resting of the brainstem on the skull base: reduction of the prepontine cistern (< 5 mm)
- Subsidence of the brainstem: small mamillopontine distance (< 6.5 mm)
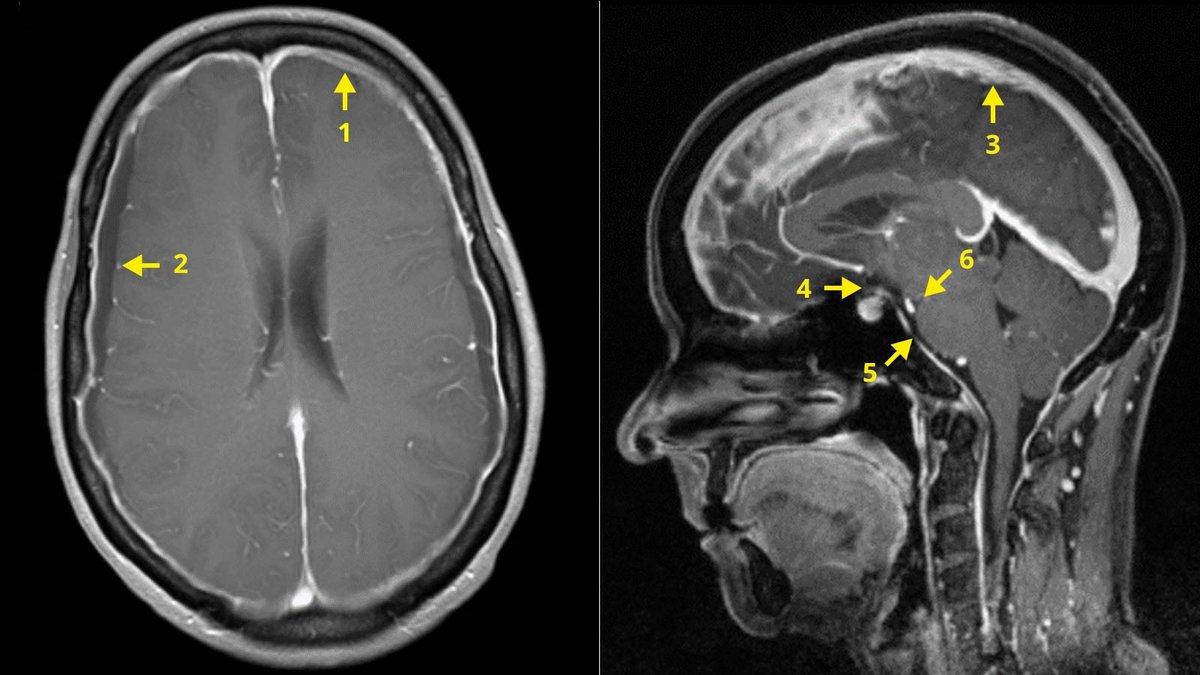
Based on these criteria, the probability of the presence of CSF leak can be calculated and classified as "low", "intermediate" or "high". Even these secondary signs of the disease (the cause is a tear in the spinal meninges in the back and not in the head itself) can be easily explained by thinking of the outflow of CSF and the brain then subsiding while standing.
What are the challenges in diagnosing this disease?
The initial question is: Is cerebrospinal fluid actually leaking through a crack in the dura?
This first needs to be confirmed with certainty. This is usually done by magnetic resonance imaging (MRI). If the findings are negative, a myelography, i.e. a radiological contrast image of the spinal canal, is performed. In addition to conventional myelography, a combination with myelo-computed tomography (myelo-CT) is also possible. If direct detection is not possible, the diagnosis can be confirmed indirectly using other methods, such as ultrasound of the optic nerve or measurement of the outflow resistance of the CSF. In this way, one knows with relative certainty that CSF is really draining.
The second question is even more important: Where exactly is the CSF fistula located, i.e. the defect in the dura from which the CSF escapes?
The most challenging part is actually finding this tiny tear and localizing it to the millimeter throughout the spine. It is precisely at this point that many examinations in other clinics fail, since conventional examinations usually conceal the leak. In addition, there are so-called "false-localizing signs", i.e. signs that are misleading.
We have developed a special step-by-step diagnostic protocol at Inselspital to answer both questions, which is performed with enormous care and in a highly standardized manner by a specialized and experienced neuroradiologist. Depending on the findings, individual steps can be skipped or additional examinations can be ordered.
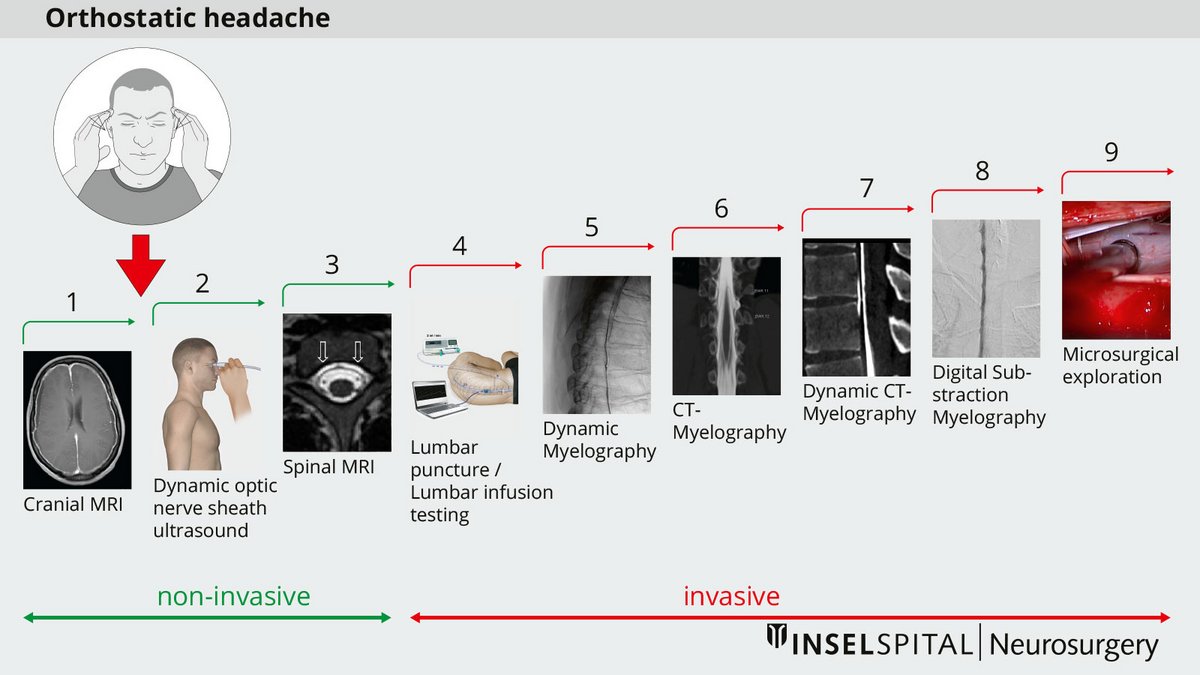
- Special sequences of cranial and spinal MRI
- Dynamic (standing and lying) ultrasound examination of the optic sheath
- Spinal MRI with intrathecal contrast imaging (in selected cases)
- Lumbar puncture with opening pressure and computerized infusion test.
- Dynamic myelography with special tilting table, if necessary intubated as digital subtraction myelography
- Post-myelo computed tomography with early images and late images if necessary
- Dynamic myelo-computed tomography of the target region with special technique *
- Digital subtraction myelography
- Microsurgical exploration
How is a CSF leak treated?
- Bed rest and caffeine (only during the initial stage for a few days).
- Blood patch (2–3 times)
- Surgery
Blood patch
If no spontaneous closure of the CSF fistula occurs through bed rest, the next step is a so-called blood patch. In this procedure, the patient's own blood, which was taken from a vein shortly beforehand, is injected into the space around the spinal cord membranes (epidural space). The blood patch is usually applied to the lower back at the level of the 3rd/4th lumbar vertebra. If necessary, the treatment is repeated. The effect of the blood patch comes not from gluing the hole shut, but from compressing the dural sac, which prevents as much cerebrospinal fluid from flowing from the head into the spinal dural sac when the patient stands up or sits down. In the short term, therefore, a blood patch nearly always improves symptoms, even if it is placed far from the leak. This minimally invasive procedure is very often successful.
If relief from symptoms is not achieved even after 2 blood patch treatments, surgical closure of the CSF leak should be performed because otherwise the headache may progress to a chronic stage with increasing involvement of cranial nerves and more severe vegetative symptoms.
What is the surgical procedure for a CSF leak?
If the CSF leak does not close after bed rest and blood patch, or in cases of large fistulas with significant symptoms, the CSF fistula is closed surgically.
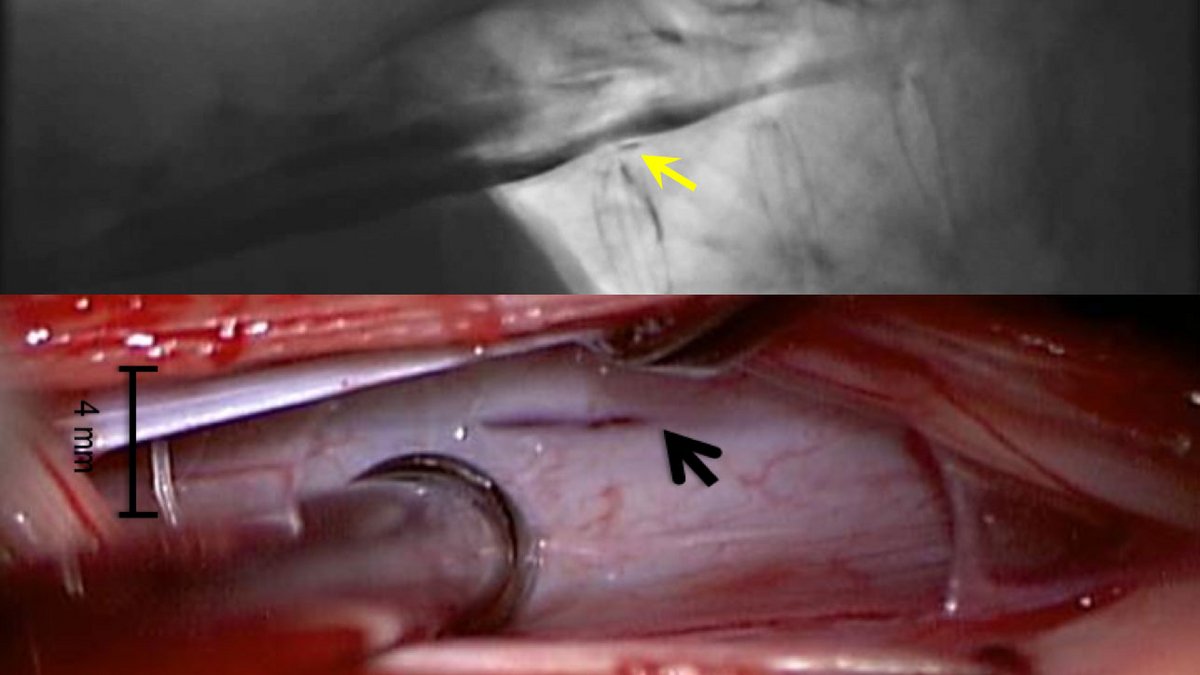
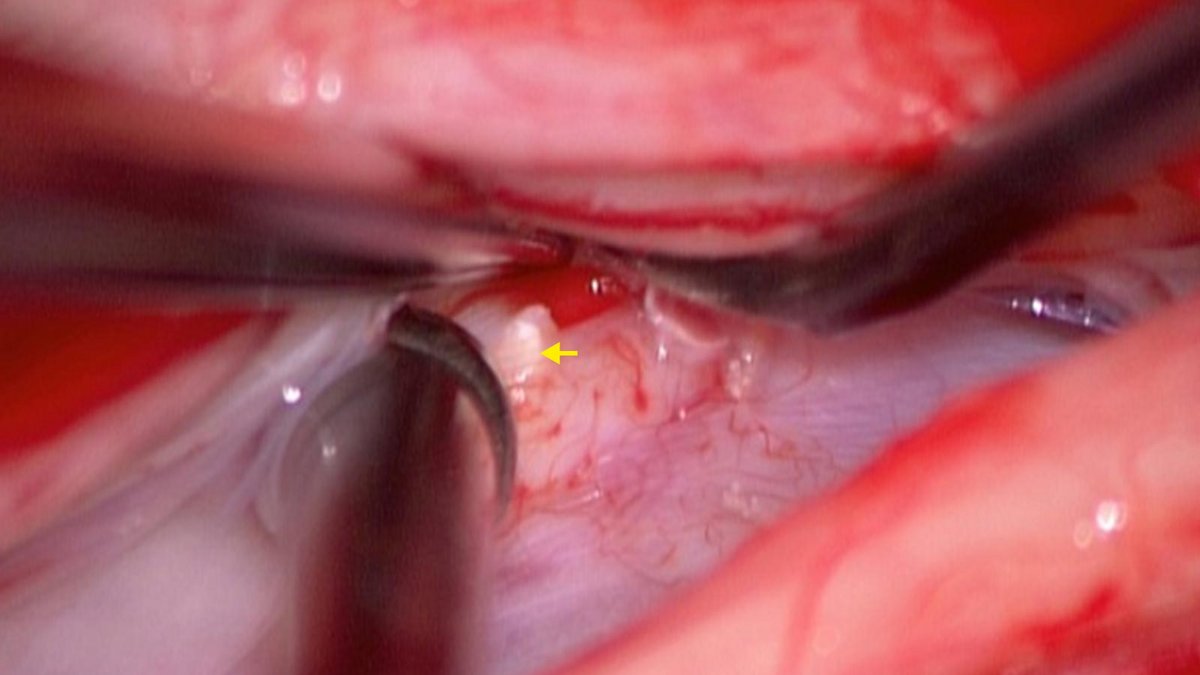
We have developed a standardized microsurgical technique for closure at Inselspital based on our experience. A 5 cm skin incision is used to perform a unilateral fenestration in the vertebral arch, leaving the vertebral process and the opposite side intact. Our specialists at Inselspital have shown that, contrary to previous assumptions, the defect is located in the vast majority of cases as a tear of 2–3 mm in front of the spinal cord *. DThe tear is often caused by a bone spur.
For monitoring and protection of spinal cord functions, our patients are continuously monitored during surgery by special spinal cord neuromonitoring. The endoscope and a fluorescent dye help locate the leak. By suturing and taping the tear in the spinal cord skin, the fistula is closed and can grow closed again..
What determines the success of the procedure?
A prerequisite for surgical treatment is the preceding exact localization of the fistula. Microsurgical treatment is then very successful. As a rule, the symptoms improve significantly immediately after the procedure or have disappeared completely. Treatment at the chronic stage is more difficult, but possible. Chronic CSF loss and surgical closure of the leak may result in scarring of nerves, and temporary or permanent CSF excess pressure may remain because the body's own breakdown of the cerebrospinal fluid has already partially atrophied. Therefore, timely diagnosis and surgical therapy is important, especially if there is no improvement after blood patch treatment.
What are the complications of this procedure?
Given the surgeon's proven microsurgical experience on the spinal cord and special functional monitoring during the operation, the complication rate is very low. The success rate for sealing is high, nevertheless in about 6% of patients a second operation has to be performed to close the leak completely watertight.
Why you should seek treatment at Inselspital
Inselspital is one of the three largest centers in Europe for cerebrospinal fluid leakage syndrome and has many years of experience in the diagnosis and treatment of this rare condition.
In recent years, we have gained important insights:
- The diagnosis is often overlooked. Specialized diagnostic procedures and a structured step-by-step approach are not widely known in many places.
- The course is often benign, with a high rate of spontaneous healing. However, if the dural leak does not close relatively quickly (spontaneously or through surgery)—or if there is a dural tear caused by a micro-spur—a chronic course with severe impairments may develop.
- Not every leak is the same. After a lumbar puncture, a leak almost always heals spontaneously. In the case of a dural slit caused by a micro-spur, spontaneous healing is significantly less common.
- The leak is often difficult to find.The leak is frequently not found during the initial evaluation. However, if symptoms persist, it is essential to continue searching for the leak. Even in our practice, a second or third round of diagnostic testing may be necessary, involving multiple MRIs and myelograms, to definitively diagnose or rule out the condition.
- Successful treatment requires two specialized teams: neuroradiological diagnostics and experienced neurosurgical teams. The leak is usually very small and well-hidden.
- Two diagnostic milestones are crucial:
- Detection of cerebrospinal fluid outside the dural sac
- Precise localization of the leak for targeted surgery
- The most common cause is a dural slit only 2–3 mm long in front of the spinal cord, usually caused by a tiny bone spur. Root pouch cysts are less common.
- Once the fistula has been located, surgery should be performed promptly. Further bed rest or repeated blood patches are usually not advisable at this point.
- After a successful operation, symptoms usually improve immediately. In about 6% of cases, an early recurrence occurs, which may require another operation.
- After a long chronic course, a temporary overpressure headache may develop. This usually resolves on its own; shunt surgery is rarely necessary.
- Rare special forms occur when cerebrospinal fluid “becomes trapped” in large radicular cysts or an enlarged dural sac. Treatment then consists of reducing the volume of the dural sac.
Further reading
Cipriani D, Rodriguez B, Häni L, Zimmermann R, Fichtner J, Ulrich CT, Raabe A, Beck J, Z'Graggen WJ. Postural changes in optic nerve and optic nerve sheath diameters in postural orthostatic tachycardia syndrome and spontaneous intracranial hypotension: A cohort study. PLoS One. 2019 Oct 9;14(10):e0223484.
-
Dobrocky T, Mosimann PJ, Zibold F, Mordasini P, Raabe A, Ulrich CT, et al. Cryptogenic Cerebrospinal Fluid Leaks in Spontaneous Intracranial Hypotension: Role of Dynamic CT Myelography. Radiology, 289(3), 766–772.
-
Beck J, Raabe A, Schievink WI, et al. Posterior Approach and Spinal Cord Release for 360° Repair of Dural Defects in Spontaneous Intracranial Hypotension. Neurosurgery. 2019;84(6):E345-E351.